Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 2 - Mar. / Apr. of 2007
Vol. 40 nº 2 - Mar. / Apr. of 2007
|
ORIGINAL ARTICLE
|
|
Ultrasound findings in thyroiditis |
|
|
Autho(rs): Ilka Yamashiro, Osmar de Cássio Saito, Maria Cristina Chammas, Giovanni Guido Cerri |
|
|
Keywords: Ultrasound, Thyroid, Thyroiditis |
|
|
Abstract:
IMD, Radiologist, Master in Health Sciences by Hospital Heliópolis Post-Graduation Course, São Paulo, SP, Professionalizing Practice at Setor de Ultra-sonografia do Instituto de Radiologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil
INTRODUCTION Thyroiditis is a generic term including an array of clinicalentities affecting the thyroid gland. The thyroiditis may present infectious, autoimmune, traumatic,postradiotherapy, drugs use, and other etiopathogenies. On thegrounds of etiopathogeny and clinical findings, eight diseasespresent with thyroiditis picture: 1) Hashimoto thyroiditis;subacute lymphocytic thyroiditis; 3) subacute granulomatousthyroiditis (De Quervain's disease); 4) postpartum thyroiditis;5) infectious thyroiditis 6) toxic thyroiditis; 7) actinicthyroiditis; 8) Riedel's thyroiditis. Subacute and chronic thyroiditis refer to inflammation of thethyroid gland parenchyma where serum thyroglobulin, T3 and T4levels increase. For this reason, during the initial phase of thedisease, the thyroiditis progresses with thyrotoxicosis. Afterthe first weeks, the damages to follicular cells inhibit thehormonal synthesis, resulting in hypothyroidism. In this phase,subacute thyroiditis is a self-limited condition and the glandtissue regenerates. On the other hand in the chronic, autoimmunethyroiditis (Hashimoto) this phase is continuous and progressesto hypothyroidism. The objective of the present study was to evaluate sonographicfeatures of thyroid gland in patients with thyroiditis.
MATERIALS AND METHODS During a nine-month period, 38 patients previously diagnosedwith thyroiditis by the Ultrasound Unit of Instituto deRadiologia do Hospital das Clínicas da Universidade deSão Paulo, São Paulo, SP, Brazil, were studied. Ofthese patients, 36 were female, with ages ranging between 17 and78 years (mean age 47.5 years). The following variables were observed and studied: thyroidvolume, echogenicity, echotexture, and the presence of level VIchain lymph nodes (pre-tracheal, the preferential site of thyroiddrainage), besides the gland dimensions.
RESULTS In our casuistic, the greatest majority of patients (36; 94.7%) were female. Thirteen patients (34.2%) presented with goiter (glandular volume > 14.4 cm³). Ultrasound analysis showed heterogeneous echotexture with diffuse hypoechogenicity in 37 (97.3%) of the 38 thyroid glands (Table 1).
All the patients presented alterations compatible withthyroiditis on laboratory tests. Causal factor or factors could not be determined because ofthe absence of previous studies performed in our Service. Also,it is important to note that ultrasound findings in thyroiditis,especially in the focal ones, may overlap with those seen inother diseases. Cervical chain lymph nodes were found at level VI(pre-tracheal) in 28 patients (73.6%), all of them presentingreactional features (ovoid, with hyperechogenic central hilum).Of these 28 cases, ten patients were submitted to fine needleaspiration biopsy, and the cytological result indicatedinflammatory reaction. No case of nodule-simulating focalthyroiditis was found.
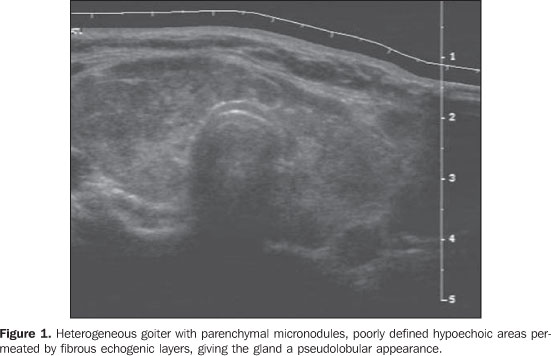
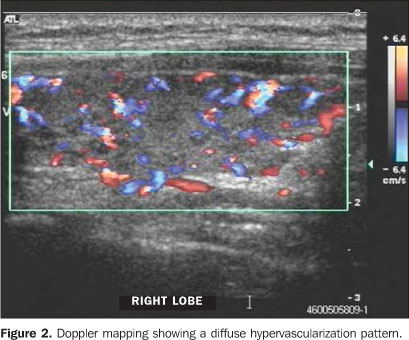
DISCUSSION The diagnosis of thyroiditis is not always easy and immediate,considering that in the initial phases of the disease specificlaboratory tests alterations are not detectable. With theprogress of imaging methods, some features such as thyroid glandsize, shape and echogenicity can be earlier and better evaluated.Consequently, ultrasonography has been useful for evaluating thethyroid gland, especially in dubious cases where morphologicaland functional characteristics may suggest the actualetiopathogeny of the disease on color Doppler mapping. Some ofthese characteristics are widely recognized in the worldwideliterature. Hashimoto thyroiditis is the most frequent cause of permanent hypothyroidism in areas of adequate iodine intake, corresponding to more than 90% of cases. It is part of the spectrum of autoimmune thyroid diseases, typically affecting older women, five to eight times more frequently than men, with an approximate 15% prevalence in this latest group(1,2). At ultrasound a heterogeneous goiter with micronodules scattered throughout the parenchyma. Progressively, the thyroid gland presents an aspect of chronic hypertrophic thyroiditis with poorly defined hypoechoic areas permeated by fibrous echogenic layers, giving the gland a pseudolobular appearance (Figure 1). Doppler mapping shows a diffuse hypervascularization pattern similar to Graves' disease (Figure 2). In the later stages of the disease color Doppler shows the thyroid gland reduced in size diffusely heterogeneous due the intense fibrosis and avascularized.
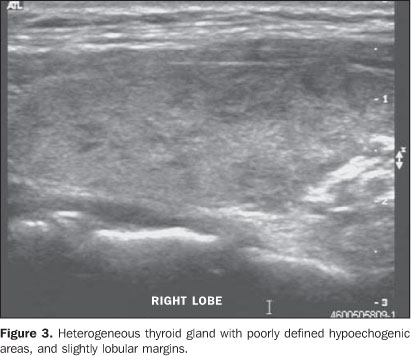
Subacute lymphocytic thyroiditis is also an autoimmune, painless disease characterized by transitory thyrotoxicosis, with lymphocytic infiltrates, similar to the Hashimoto thyroiditis (Figure 3)(1,2).
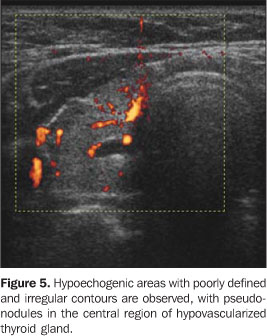
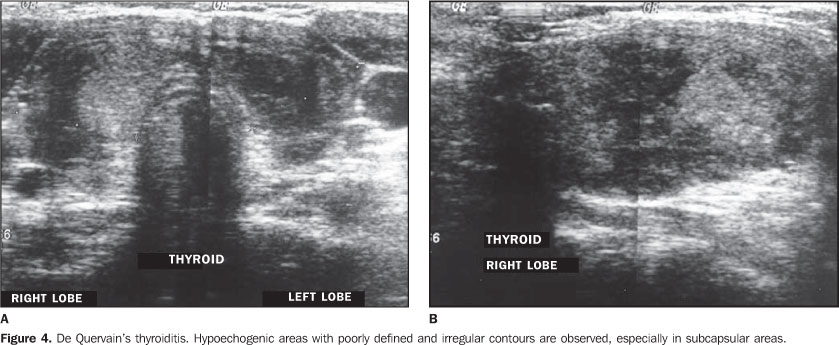
Subacute granulomatous thyroiditis (De Quervain's) also manifests with thyrotoxicosis, cervicoalgia, most frequently affecting women at a 3:1–5:1 ratio. It is a reactional, post-viral disease (Cocksackie, adenovirus, mumps, measles, etc.)(1,3,4). In the initial phase of this disease, ultrasound shows hypoechogenic areas with irregular, poorly defined margins, especially in the subcapsular zones (Figure 4). Later, pseudonodules may be observed in the central region of the thyroid gland. In the early phases, vascularization may be reduced (Figure 5).
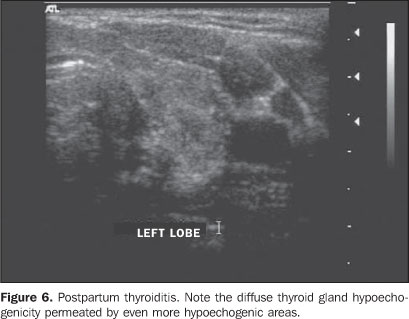
Postpartum thyroiditis is also an autoimmune process that may occur in the first year after delivery, most frequently between the second and fourth month, affecting up to 7% of women. Recurrence rates in subsequent gestations are high(5,6). At ultrasound a diffuse thyroid gland hypoechogenicity is observed, with even more hypoechogenic focal areas (Figure 6).
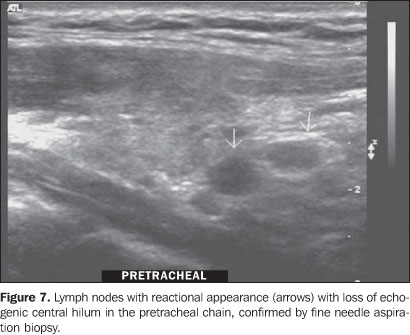
Other types of thyroiditis occur less frequently, and theinfectious ones usually are caused bybacteria(5); in cases of immunodepressedpatients, fungi and tubercle bacillus should be considered asetiological agents. B-mode ultrasound shows poorly defined,hypoechogenic foci, probably corresponding to formation ofintraparenchymal abscesses. Thyroiditis also can be associatedwith the use of interferon-2, interleukin andamiodarone(7–9). Riedel's thyroiditis is a rare chronic form of thyroiditiswhere fibrous tissue replaces the normal thyroid tissue, causinghardening and diffuse destruction of the gland, and tending toextend to the adjacent tissues. This disease may result indyspnea and dysphagia, and an association exists between Riedel'sthyroiditis and retroperitoneal fibrosis, mediastinal fibrosis,pulmonary fibrosis, sclerosing cholangitis, pseudo-tumor of theorbit, etc.(1,6). At ultrasound, the thyroidgland is shown as a hypoechogenic mass infiltrating into theadjacent musculature. In the greatest majority of cases, the diagnosis is based on clinical findings and laboratory tests results, and ultrasound is an important tool in the morphological evaluation of the thyroid gland, corroborating the diagnosis, and also providing additional information regarding the disease extent and mainly regarding cervical chain lymph node involvement (level VI, pre-tracheal, the preferential site of thyroid drainage)(10). Although these lymph nodes are not mentioned in current studies, they may be confused with thyroid isthmus nodules. Fine needle aspiration biopsy demonstrated that these lymph nodes were of reactional inflammatory origin (Figure 7).
Our casuistic matches the literature, the majority of ourpatients being female, with 97.3% of the thyroids evaluatedpresenting diffusely hypoechogenic and heterogeneous atexamination (with poorly defined, hypoechogenic foci andpermeated with echogenic layers), as well as the presence ofcervical chain lymph nodes in 73.6% of cases. However, only 34.2%of the patients presented with goiter in the moment ofexamination. It is important to note that patients must be carefullyevaluated in order to avoid that the presence of any nodule ismissed in the middle of a heterogeneous parenchyma, since 20% ofpatients with Hashimoto thyroiditis may develop malignant nodulesor thyroid lymphomas(11). Lymph nodesevaluation, especially by means of B-mode morphological imagingis also relevant, since these lymph nodes may correspond topreviously unknown malignant processes(12).About 10%–15% of Hashimoto thyroiditis course withlymphadenomegaly of questionable nature(9).
CONCLUSION One may conclude that ultrasound findings of glandularheterogeneity and hypoechogenicity, associated with cervicalchain (level VI) lymph nodes, are extremely useful in thediagnosis of thyroiditis when correlated with laboratory andclinical tests.
REFERENCES 1. Goldman L, Bennet JC. Cecil Textbook of medicine. 21st ed. Philadelphia: WB Saunders, 2000. [ ] 2. Lazarus JH. Silent thyroiditis and subacute thyroiditis. In: Braverman LE, Utiger RD, editors. The thyroid: a fundamental and clinical text. 7th ed. Philadelphia Lippincott-Raven, 1996;577–591. [ ] 3. Basgoz N, Swartz MN. Infections of the thyroid gland. In: Braverman LE, Utiger RD, editors. The thyroid: a fundamental and clinical text. 7th ed. Philadelphia: Lippincott-Raven, 1996;1049–1056. [ ] 4. Solbiati L, Charboneau JW, James EM, Hay ID. The thyroid gland. In: Rumack CM, Wilson SR, Charboneau JW, editors. Diagnostic ultrasound. 2nd ed. St. Louis: Mosby, 1998;703–729. [ ] 5. Bokhari R, Bhatara VS, Bandettini F, McMillin JM. Postpartum psychosis and postpartum thyroiditis. Psychoneuroendocrinology 1998;23: 643–650. [ ] 6. Chammas MC, Saito OC, Cerri GG. Tireóide. In: Saito OC, Cerri GG, organizadores. Ultra sonografia de pequenas partes. 2ª ed. Rio de Janeiro: Revinter, 2004;75–114. [ ] 7. Preziati D, La Rosa L, Covini G, et al. Autoimmunity and thyroid function in patients with chronic active hepatitis treated with recombinant interferon alpha-2a. Eur J Endocrinol 1995;132: 587–593. [ ] 8. Roti E, Minelli R, Giuberti T, et al. Multiple changes in thyroid function in patients with chronic active HCV hepatitis treated with recombinant interferon-alpha. Am J Med 1996;101: 482–487. [ ] 9. Roti E, Minelli R, Gardini E, Bianconi L, Braverman LE. Thyrotoxicosis followed by hypothyroidism in patients treated with amiodarone. A possible consequence of a destructive process in the thyroid. Arch Intern Med 1993;153:886–892. [ ] 10. Som PM, Brandwein. Lymph nodes. In: Som PM, Curtin HD, editors. Head and neck imaging. 4th ed. St. Louis: Mosby, 2003;1880–1883. [ ] 11. Takashima S, Takayama F, Wang Q, Kobayashi S, Sone S. Thyroid metastasis from rectal carcinoma coexisting with Hashimoto's thyroiditis: gray-scale and power Doppler sonographic findings. J Clin Ultrasound 1998;26:361–365. [ ] 12. Senchenkov A, Staren ED. Ultrasound in head and neck surgery: thyroid, parathyroid, and cervical lymph nodes. Surg Clin North Am 2004;84: 973–1000. [ ]
Received May 31, 2006.
* Study developed in the Ultrasound Unit of Instituto de Radiologia do Hospital das Clínicas da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil. |
|

{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554