Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 41 nº 6 - Nov. / Dec. of 2008
Vol. 41 nº 6 - Nov. / Dec. of 2008
|
CASE REPORT
|
|
Giant oesophageal liposarcoma: case report |
|
|
Autho(rs): Richard Page, Ranjeet Narlawar, John Holemans, John Gosney, Richard Warwick, Hany Elsayed |
|
|
Keywords: Liposarcoma, Oesophagus, Computed tomography scan |
|
|
Abstract: IChM, FRCS(CTh), Medical Doctor of the Department of Cardiothoracic Surgery of the Liverpool Heart and Chest Hospital NHS Trust, Liverpool, United Kingdom
INTRODUCTION Gastrointestinal liposarcomas are rare tumours, with oesophagus being the least common site. Imaging findings of very few cases have been described in literature. These tumours have varied imaging appearances. Although imaging can not accurately differentiate between benign and malignant tumours, it has a pivotal role in staging and management of liposarcomas, especially oesophageal due to their close proximity to mediastinum and spine. We present imaging findings with histological correlation of such a rare entity.
CASE REPORT A 66 year old man presented with chronic cough and mucoid expectoration. A chest x-ray was performed, which revealed a large posterior mediastinal tumour (Figure 1). The lung fields were normal. Computed tomography (CT) scan of the chest and abdomen was performed for further characterisation. CT scan showed a large, well defined, mixed density, but predominantly fat density mass in the posterior mediastinum. The mass was engulfing the oesophagus all around (Figure 2). There was mass effect and displacement of the posterior wall of the left atrium. The tumour was encasing the thoracic aorta for at least 180 degrees. The fat plane between the mass and the adjacent mediastinal structures was effaced. More distally, the mass caused complete collapse of the oesophageal lumen. There was no mediastinal or hilar lymphadenopathy. The lung fields were normal. No abnormality detected within the abdomen. Due to mixed nature of the lesion, possibility of the malignant lesion in the posterior mediastinum was raised.
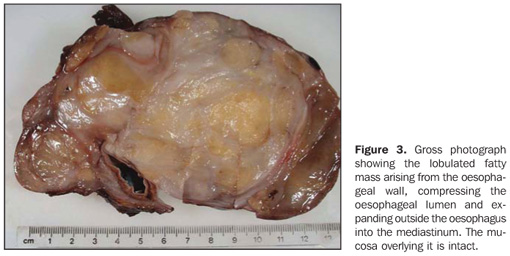
On further questioning, he gave the history of few months of difficulty in swallowing for which upper gastrointestinal endoscopy was performed in other hospital. It showed changes of Barrett's oesophagus; no other significant abnormality was noted. Patient underwent thoracotomy. The mass was well encapsulated, it was encircling the oesophagus, was seen free from the surrounding mediastinal structures. Complete removal of the tumour with distal oesophagectomy and oesophagogastrectomy was performed. Post operative recovery was uneventful. Examination of the resected specimen revealed a fatty tumour that clearly arose from the submucosal region of the oesophageal wall, growing and expanding outside the oesophagus to encircle it and form a thinly-encapsulate mass 150 × 140 × 75 mm in diameters (Figure 3). The mucosa overlying the tumour was normal.
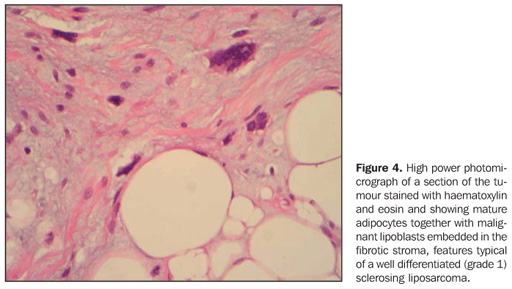
Microscopic examination (Figure 4) showed lobules of fatty tissue separated by a collagenous and myxoid stroma. There was marked variation in the size of the adipocytes with scattered uni- and multivacuolated lipoblasts, some of them apparently entrapped within the fibrous septa. These lipoblasts had large, atypical, hyperchromatic nuclei. Mitotic figures were present, numbering between 5 and 10 per ten high-power microscopic fields, but there was no necrosis. These features indicated the tumour to be a well differentiated (grade 1) liposarcoma of sclerosing subtype. The thin capsule of the lesion was intact and excision was considered complete.
DISCUSSION Gastro-intestinal (GI) liposarcomas constitute about 0.1% to 5.8% of all the liposarcomas at autopsy and the oesophagus is the least common site. Oesophageal liposarcomas constitutes 1.2% to 1.5% of all GI liposarcomas(1). First case was reported in 1983(2) and since then only 15 other cases have been reported in the world literature so far. They are slowly growing tumours arising from the mucosa or submucosal soft tissue layers of the oesophagus. Pathologically, the tumour is either well-differentiated liposarcoma or myxoid histotype(1). There are varied clinical presentations of oesophageal liposarcoma. Mean age varies between 43 to 73 years and male sex being affected slightly more than female sex. Most patients complain dysphagia. They may remain asymptomatic, until the tumour grow to a very large size and cause invasion or mass effect on the adjacent structures. Weight loss, fever, odynophagia, respiratory distress, epigastric pain(3) which may or may not be associated with gastro-intestinal bleeding. There has been even a case report where there was oral protrusion of the tumour. CT scan features are similar to those reported in liposarcoma elsewhere in the body. Due to fatty nature of this lesion, CT scan mostly reveals a large, predominantly fat density lesion mixed with varying amount of soft tissue. Most of the reported cases showed intra or extra luminal polypoid mass(1,4,5). Proximal, mid as well as distal oesophageal involvement have been reported. Presence of fat may indicate lipomatous tumour such as lipoma, atypical lipoma and liposarcoma. CT scanning not only is helpful in characterising the lesion but also helps in studying the mediastinal structures in detail, as these tumours are known to cause compression or invasion of the adjacent structures. Although, CT scanning remains the most important diagnostic modality, other modalities like barium swallow, trans-oesophageal ultrasound scanning, endoscopy, magnetic resonance imaging (MRI) may also be performed. MRI may show high signal intensity within the fatty tissue on T1 weighted images, which suppresses on in phase and out of phase imaging or on fat suppressed images(6). In addition, MRI helps in better assessment of involvement of the adjacent structures as compared with CT scanning. Poorly differentiated tumours, which pathologically tend to be more cellular with less fat per cell component, are likely to have high CT numbers. CT number is not sufficient to distinguish well-differentiated liposarcoma from benign lipoma(7) and histopathologic examination is always necessary as much for diagnosis as prognosis in these cases(8). Imaging modalities are limited in their capability to tell the malignant potential of the tumour. Hence complete resection is most commonly advised treatment option(6,9,10). There are various surgical options. They vary from endoscopic resection, simple enucleation to more invasive transthoracic, trascervical or transgastric approach. Survival depends on histologic subtypes, grade of malignancy, location and surgical radicality(4). Survival between 7 months to 104 months has been reported. A previous study reported a case of recurrence 25 years after the first episode in a 68 year old woman(11). In conclusion, oesophageal liposarcomas are rare tumours with varied presentation. Even if CT and MRI features are typical, they are not unique. There are various differential diagnoses of fat containing masses in the mediastinum. Surgical resection is the treatment of choice and only histological examination can make confident diagnosis. Acknowledgement The authors would like to acknowledge the contribution of Mr Mike Poullis and Dr Klaus Irion.
REFERENCES 1. Yang B, Shi PZ, Li X, et al. Well-differentiated liposarcoma of esophagus. Chin Med J (Engl). 2006;119:438–40. [ ] 2. Mansour KA, Fritz RC, Jacobs DM, et al. Pedunculated liposarcoma of the esophagus: a first case report. J Thorac Cardiovasc Surg. 1983;86:447–50. [ ] 3. Liakakos TD, Troupis TG, Tzathas C, et al. Primary liposarcoma of esophagus: a case report. World J Gastroenterol. 2006;12:1149–52. [ ] 4. Mica L, Gianom D, Bode B, et al. Rare cause of dysphagy: giant polypoid esophageal well-differentiated liposarcoma. Case Rep Gastroenterol. 2007;1:7–14. [ ] 5. Di Mascio L, Gamble L, Wajed S, et al. Intussuscepting giant liposarcoma of the oesophagus. J Postgrad Med. 2006;52:231–2. [ ] 6. Chung JJ, Kim MJ, Kim JH, et al. Imaging findings of giant liposarcoma of the esophagus. Yonsei Med J. 2003;44:715–8. [ ] 7. Taira N, Kinoshita S, Miyake T, et al. Primary liposarcoma of the anterior mediastinum – case report and review of literature. Jpn J Thorac Cardiovasc Surg. 1998;46:450–4. [ ] 8. Bonnette P, Jouan J, Colchen A, et al. Myxoid liposarcoma of the mediastinum. Rev Mal Respir. 2000;17:109–11. [ ] 9. Boggi U, Viacava P, Naccarato AG, et al. Giant pedunculated liposarcomas of the esophagus: literature review and case report. Hepatogastroenterology. 1997;44:398–407. [ ] 10. Bréhant O, Pessaux P, Hennekinne-Mucci S, et al. Giant pedunculated liposarcoma of the esophagus. J Am Coll Surg. 2004;198:320–1. [ ] 11. Beaudoin A, Journet C, Watier A, et al. Giant liposarcoma of the esophagus. Can J Gastroenterol. 2002;16:377–9. [ ]
Received September 9, 2008. Accepted after revision September 22, 2008.
* Study developed at Liverpool Heart and Chest Hospital NHS Trust, Liverpool, United Kingdom. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554