Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 41 nº 5 - Sep. / Oct. of 2008
Vol. 41 nº 5 - Sep. / Oct. of 2008
|
WHICH IS YOUR DIAGNOSIS?
|
|
Which is your diagnosis? |
|
|
Autho(rs): Renato Tavares Daher, Sérgio Daher, Murilo Tavares Daher, Ricardo Tavares Daher, Marcelo Eustáquio Montandon Júnior, Cristiano Montandon |
|
|
IMD, Resident in Radiology and Imaging Diagnosis at Hospital das Clínicas, Universidade Federal de Goiás (HC-UFG), Goiânia, GO, Brazil. E-mail: renatodaher@uol.com.br
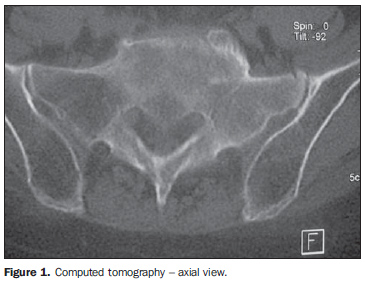
A female, Caucasian, 76-year-old patient reported the onset, approximately three weeks ago, of an intense, diffuse lumbar pain, irradiating over the lower limbs up to the knees. The pain did not decrease with rest and presented only a mild improvement with analgesic and non-hormonal anti-inflammatory drugs. The patient reported a previous history of rectal neoplasm treated with surgery and radiotherapy six months ago. At clinical examination, the patient presented pain at palpation and movement of the lumbar region, negative Lasègue's sign, with no motor or sensitivity deficit. Plain radiography (unshown), computed tomography (Figure 1) magnetic resonance imaging (Figures 2, 3 and 4) and, subsequently, open biopsy and histology of the sacrum were performed.
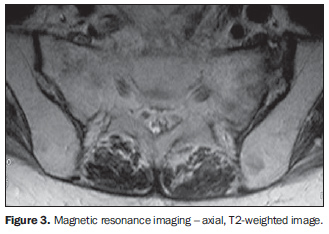
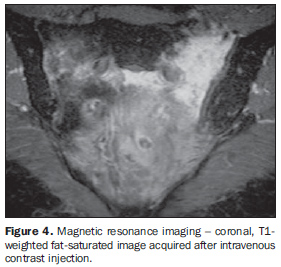
Images description Figure 1. Computed tomography - axial view demonstrating anterior cortical fracture of the left sacral wing associated with osteocondensation with adjacent cortical thickening. Figure 2. Magnetic resonance imaging - sagittal, T1-weighted image demonstrating small fracture traces characterized by hypointense signal subjacent to disk spaces S1-S2 and S2-S3. Figure 3. Magnetic resonance imaging - axial T2-weighted image demonstrating fracture traces on the spongeous bone of the sacral wings, parallel to the sacroiliacal joints associated with adjacent medullary bone edema. Figure 4. Magnetic resonance imaging - coronal T1-weighted fat-saturated image acquired after intravenous contrast injection. Note the intense, asymmetrical contrast uptake in the sacral bone marrow beside the fracture traces, most noticeable at left, additionally to another horizontal component subjacent to the disk S1-S2, characterizing the typical H-shaped fracture. Diagnosis: Sacral insufficiency fractures.
COMMENTS Stress fractures affect patients with no history of trauma, and are classified into subgroups as follows: fatigue fractures - in a normal bone submitted to a repetitive effort; or insufficiency fracture - occurring during normal stress on a generally osteopenic bone, likewise in the present case(1). Firstly described in 1982 by Lourie, sacral insufficiency fracture is a frequent complication of osteoporosis, affecting 2% to 4% of caucasian women with > 60 years, constituting a relevant cause for pelvic and/or lumbar pain(2). Postmenopausal osteoporotic women submitted to pelvic radiotherapy are even more prone to this complication, like in the present case, despite the absence of actinic alterations as demonstrated by biopsy(3). The load exerted by the body over the sacrum through the spine, associated the mechanical strength transferred by the deambulation to the sacrum through the sacroiliacal joints, cause bilateral fractures on the sacral wings, parallel to these joints, and a third fracture on the same bone interconnecting them and forming the typical H-shaped fracture(4). Hip fractures, particularly in the pubic branches, are frequently associated, which has not been observed in the present case. Main clinical characteristics are pelvic and lumbar pain, impaired deambulation and, rarely, neurological and medullary compression symptoms(2,3), likewise in the case presently described. The diagnostic suspicion is based on an association of clinical data, physical examination and imaging findings. Plain radiography of the pelvis can hardly demonstrate the fracture trace. The most frequent radiographic finding is osteopenia(3). The most easily noticeable tomographic findings are radiolucent lines and sclerotic bands on the sacral wings, besides anterior cortical fractures of the sacrum, typically found in these cases(1,2,5). Bone scintigraphy demonstrates the H-shaped radiopharmaceutical uptake. Magnetic resonance imaging presents 100% sensitivity and 83% specificity(3), with T1-weighted sequences demonstrating hypointense signal on bilateral fracture traces parallel to the sacroiliacal joints, and a third perpendicular line interconnecting them, forming a H-shaped fracture(5,6). T2-weighted sequences demonstrate medullary edema, which may hide the fracture trace early in the first months(2,3,5). Paramagnetic contrast-enhanced T1-weighted fat-suppressed sequences have shown to be more sensitive for identifying fracture traces(1,3,5). The evaluation of coronal, oblique images of the sacrum provide useful information for the diagnosis. In patients with a known neoplasm, secondary implant is the primary differential diagnosis to be initially considered, since disabling pain is also a typical symptom of this entity. Typically in these cases, multifocal, infiltrative solid lesions can be observed affecting adjacent soft tissues, differently from sacral insufficiency fractures(5).
FINAL CONSIDERATIONS With the increased longevity and the consequent prevalence of osteoporosis, particularly amongst women, sacral insufficiency fractures tend to become an increasingly frequent diagnosis. In the present report, the authors demonstrate the relevance of recognition of the typical imaging findings by radiologists to avoid unnecessary invasive procedures.
REFERENCES 1. Keogh C, Torreggiani WC, Al-Ismail K. Musculoskeletal case 21. Insufficiency fracture of the sacrum. Can J Surg. 2002;45:92, 153. [ ] 2. Grangier C, Garcia J, Howarth NR, et al. Role of MRI in diagnosis of insufficiency fractures of the sacrum and acetabular roof. Skeletal Radiol. 1997;26:517-24. [ ] 3. Peh WC, Khong PL, Yin Y, et al. Imaging of pelvic insufficiency fractures. Radiographics. 1996; 16:335-48. [ ] 4. Mammone JF, Schweitzer ME. MRI of occult sacral insufficiency fractures following radiotherapy. Skeletal Radiol. 1995;24:101-4. [ ] 5. Blake SP, Connors AM. Sacral insufficiency fracture. Br J Radiol. 2004;77:891-6. [ ] 6. Blomlie V, Lien HH, Iversen T, et al. Radiation-induced insufficiency fractures of the sacrum: evaluation with MR imaging. Radiology. 1993; 188:241-4. [ ] Study developed at the Spine Unit of Hospital de Acidentados de Goiânia and at Clínica Multimagem, Goiânia, GO, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554