Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 6 - Nov. / Dec. of 2009
Vol. 42 nº 6 - Nov. / Dec. of 2009
|
ORIGINAL ARTICLE
|
|
Reproducibility of ultrasonography as a method to measure abdominal and visceral fat |
|
|
Autho(rs): Angélica Lemos Debs Diniz, Raphael Alves Ferreira Tomé, Cecília Lemos Debs, Renata Carraro, Leonardo Borges Roever, Rogério de Melo Costa Pinto |
|
|
Keywords: Abdominal fat, Ultrasound, Metabolic syndrome |
|
|
Abstract:
IPhD, Permanent Professor, Post-graduation of Health Sciences at Universidade Federal de Uberlândia (UFU), Uberlândia, MG, Brazil
INTRODUCTION Metabolic syndrome is currently considered as a worldwide epidemic achieving increasing and alarming numbers, associated with high cardiovascular morbimortality rates besides increased socioeconomic costs(1-3). Several studies demonstrate the closed relation between abdominal adiposity and glucose intolerance, hyperinsulinemia, hypertriglyceridemia and arterial hypertension. Recently, it has been believed that, more than a simple association, abdominal fat, particularly the visceral one, plays a significant role in the metabolic syndrome physiopathology(1-4). Therefore, the quantification of visceral fat is important to identify those individuals with higher risk for developing metabolic syndrome and thus eligible for being submitted to earlier interventions in an attempt to reduce the impact of metabolic alterations on the cardiovascular morbimortality in such individuals(3,4). Computed tomography is the method of choice for quantifying visceral fat, but it has not been solely utilized in the diagnostic routine of patients with metabolic syndrome(5,6). Waist size and waist-hip ratio, although indirectly, constitute other methods for visceral fat evaluation(7). Magnetic resonance imaging has been proposed as an alternative method free from ionizing radiation, but the literature reports restrictions for patients with morbid obesity, claustrophobia, or metal prosthesis and pacemaker(8-10). Ultrasonography is a low cost and useful method besides not requiring radiation for evaluating visceral fat tissue(5,6,8,10). Additionally, recent publications have demonstrated similar effectiveness of both ultrasonography and computed tomography in the quantification of visceral fat(5-7). However, ultrasonography is operator-dependent, besides requiring the definition of specific anatomic landmarks and a standardized scanning technique. The present study is aimed at evaluating the interobserver variability of the sonographic method in the measurement of subcutaneous, visceral and perirenal fat by means of a standardized technique.
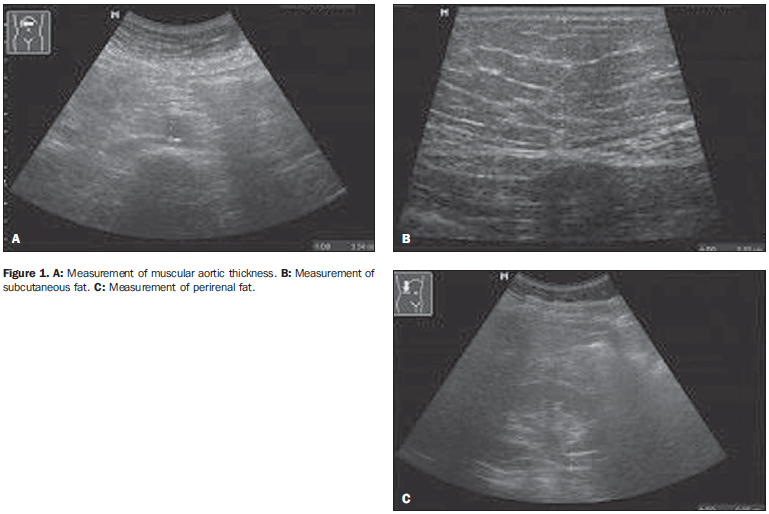
MATERIALS AND METHODS Observational study analysing abdominal and visceral fat in 50 patients by means of ultrasonography performed by two observers with a same scanning technique. The abdominal fat was quantified through the following sonographic measurements: abdominal subcutaneous, visceral and perirenal fat. The present study was developed in the Division of Ultrasonography at Hospital de Clínicas of Universidade Federal de Uberlândia, Minas Gerais, Brazil, with previous approval by the Committee for Ethics in Research of the institution. All the patients signed a term of free and informed consent. The study group included both male and female patients consecutively and randomly selected, independently from their body mass índex. The mean age of such patients was 42 years ± 12 years. The ultrasonography scans were performed by two radiologists who utilized a same, previously standardized scanning technique. Each of the patients was evaluated on the same day by two investigators who were not aware of the results of each other, in order to avoid samples contamination. A Versa Pro (Siemens; Erlangen, Germany) equipment was utilized with electronic, linear 7.5 MHz and convex, 3.5 MHz transducers. All the scans were performed with the patient under 12-hour fasting, lying in dorsal decubitus and maximum abduction of the right arm. The measurement of subcutaneous fat was performed with a linear 7.5 MHz transducer transversely positioned 1 cm above the umbilical scar, without exerting any pressure over the abdomen in order to avoid underestimation of the measurement. The subcutaneous thickness corresponded to the distance in centimeters between the skin and the outer surface of the fascia of the abdominal muscles. For the visceral fat, a 3.5 MHz transducer was also transversely positioned 1 cm above the umbilical scar on the abdominal midline, without exerting any pressure over the abdomen. The visceral fat thickness corresponded to the measurement in centimeters between the internal surface of the abdominal rectus muscle and the posterior aortic wall in the abdominal midline, during expiration. The perirenal fat was measured with a convex 3.5 MHz transducer longitudinally positioned on the axillary midline, with identification of the right kidney image. The perirenal fat thickness corresponded to the distance in millimeters between the lateral border of the kidney and the iliopsoas muscle surface adjacent to the middle third of the right kidney (Figure 1). Statistical analyses Descriptive statistical analysis was utilized for sociodemographic characterization and for calculating mean and standard deviation of the values found for the three measurements performed by the two investigators. The data normality was evaluated by the Lilliefors test. The Student t-test was utilized to compare the measurements performed by the two investigators for the subcutaneous and visceral fat variables, and the Mann-Whitney test, for perirenal fat. The intraclass correlation coefficient and respective confidence interval(11) were utilized for determining the reproducibility of the measurements obtained by the two investigators. Additionally, the Bland-Altman plot(12) was utilized for evaluating the interobserver agreement. The level of statistical significance was defined as p < 0.05.
RESULTS Mean values and respective standard deviations were 2.64 cm ± 1.37 for subcutaneous fat thickness, 6.84 cm ± 2.38 for visceral fat thickness, and 4.89 mm ± 2.6 for the perirenal fat thickness. No statistically significant difference was observed among the measurements of subcutaneous, visceral and perirenal fat performed by the investigators 1 and 2 (p = 0.7141, 0.7286 and 0.6368, respectively), indicating a good level of interobserver agreement (Figure 2). Such good interobserver agreement can be confirmed on Figures 3, 4 and 5 regarding subcutaneous, visceral and perirenal fat, respectively.
Figure 3 (subcutaneous fat) demonstrates that most of times, the values remained between mean ± one standard deviation, and in only seven patients the values were > one standard deviation. The mean difference was very low, i.e., -0.10 cm and standard deviation, 0.31 cm, showing excellent interobserver agreement. Additionally, the maximum and minimum values for the differences were, respectively, 0.9 and -0.9. As regards the interobserver agreement for the visceral fat variable (Figure 4), an excellent level was observed, with the majority of values remaining between the mean and one standard deviation. The differences were a little higher as compared with the subcutaneous fat, i.e., the mean difference was 0.16 cm and standard deviation, 0.93 cm. Measurements for eleven patients remained above this threshold. The measurements performed by the two investigators for perirenal fat also presented a good interobserver agreement, with the majority of values remaining between the mean and one standard deviation (Figure 5). The mean difference was -0.14 mm and standard deviation, 1.39 mm. Measurements for twelve patients remained above this threshold. As regards the interobserver reproducibility, intraclass correlation coefficient of 0.97 was observed (confidence interval [CI] 95%: 0.96-0.99, p < 0.01) for subcutaneous fat, 0.91 (CI 95%: 0.86-0.95, p < 0.01) for visceral fat, and 0.63 (CI 95%: 0.44-0.78, p < 0.01) for perirenal fat. An excellent interobserver reproducibility is observed for subcutaneous and visceral fat, and satisfactory correlation for perirenal fat.
DISCUSSION Considering the current worldwide epidemics of metabolic syndrome, and the knowledge on the obesity's impact on the morbidity and mortality resulting from cardiovascular events, it is increasingly necessary to develop diagnostic methods capable of evaluating and quantifying the distribution of the body fat, particularly the visceral fat(2-4,13,14). It is known that fat may accumulate in several abdominal compartments, including the epiploon, viscera such as the liver, as well as in the retroperitoneal region, including the perirenal region. Ultrasonography has shown to be a practical, effective and low-cost method besides not requiring ionizing radiation(5,7,9,10,14,15). Such factors, in association with its relevant role in the identification of individuals with increased central adiposity, may represent an important step towards the future possibility of selecting patients at high risk for developing metabolic syndrome, aiming at allowing an early intervention, thus minimizing the impact resulting from the complications of this condition(3,8,13,16). In the present study, ultrasonography has demonstrated to be highly reproducible and capable of measuring the thickness of subcutaneous, visceral and perirenal fat. Among the several advantages of ultrasonography, it is important to observe that high availability, low cost and reproducibility are factors that meet the needs of developing countries which may utilize this method in public health measures to reduce social costs(7,9,14,15,17,18). The study of abdominal fat by means of ultrasonography was first undertaken early in the nineties by Armellini et al. by comparison of sonographic and computed tomography findings in a group of 50 obese women. The sonographic findings presented a good correlation with the computed tomography findings (r = 0.66, p < 0.001), corroborating the hypothesis that ultrasonography could be useful in the assessment of abdominal fat(15). Later studies have demonstrated a poor correlation between sonographic and tomographic findings for measurement of visceral fat(7,14,17,18). However, study developed by Stolk et al. concluded that the low reliability of the measurements of visceral fat by ultrasonography would be a result from failures in a strict standardization of visceral measurements such as inappropriate transducer positioning, pressure on the abdomen and measurements at different phases of the respiratory cycle(17). Such factors may impair the quantification of abdominal fat, leading to poorly reproducible results. This fact has not been observed in the present study that has been developed in compliance with strict standardization for measurement of abdominal fat. Abdominal computed tomography is considered as the gold standard in the determination of visceral fat, since this method can differentiate subcutaneous from visceral fat, besides being highly reproducible(5-7,14). The advantage of computed tomography and magnetic resonance imaging in the evaluation of abdominal fat is the fact that these methods do not depend on the operator ability to identify the structures during the examination, besides not being influenced by the pressure exerted by the transducer over the patient's abdomen during the measurements. However, the ionizing radiation present in computed tomography and the high cost and long acquisition time of magnetic resonance imaging represent unfavorable aspects in the utilization of such methods in the routine for quantifying abdominal fat, considering that ultrasonography presents an optimum reproducibility(6,7,10). The present study has demonstrated a high interobserver agreement and thus the ultrasonography reproducibility in the quantification of abdominal fat by means of measurements of subcutaneous, visceral and perirenal fat, with excellent CI for the first two types of fat, and a reasonable CI for perirenal fat - an already expected result because of the higher technical difficulty in the evaluation of the perirenal fat. Additionally, the perirenal fat is measured in millimeters, becoming more susceptible to biometric errors. The development of the present study only was possible because the description and utilization of a strict protocol for measurement of abdominal fat. It is important to mention some technical limitations, since they may pose some difficulty to the performance of the US scan, limiting its reliability. Among these limitation, one may observe non-cooperation of the patient in respiratory maneuvers, utilization of inappropriate transducers and, particularly, inappropriate operator training and technique(5,17,18). Therefore, ultrasonography presented a good interobserver reproducibility in the evaluation of abdominal and visceral fat by means of measurements of the thickness of subcutaneous, visceral and perirenal fat.
REFERENCES 1. Radominski RB, Vezozzo DP, Cerri GG, et al. O uso da ultra-sonografia na avaliação da distribuição de gordura abdominal. Arq Bras Endocrinol Metab. 2000;44:5-12. [ ] 2. Timar O, Sestier F, Levy E. Metabolic syndrome X: a review. Can J Cardiol. 2000;16:779-89. [ ] 3. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1-253. [ ] 4. van der Kooy K, Seidell JC. Techniques for the measurement of visceral fat: a practical guide. Int J Obes Relat Metab Disord. 1993;17:187-96. [ ] 5. Hirooka M, Kumagi T, Kurose K, et al. A technique for the measurement of visceral fat by ultrasonography: comparison of measurements by ultrasonography and computed tomography. Intern Med. 2005;44:794-9. [ ] 6. Armellini F, Zamboni M, Robbi R, et al. Total and intra-abdominal fat measurements by ultrasound and computerized tomography. Int J Obes Relat Metab Disord. 1993;17:209-14. [ ] 7. Pineau JC, Guihard-Costa AM, Bocquet M. Validation of ultrasound techniques applied to body fat measurement. A comparison between ultrasound techniques, air displacement plethysmography and bioelectrical impedance vs. dual-energy X-ray absorptiometry. Ann Nutr Metab. 2007;51:421-7. [ ] 8. Pozzato C, Radaelli G, Dall'Asta C, et al. MRI in identifying hepatic steatosis in obese children and relation to ultrasonography and metabolic findings. J Pediatr Gastroenterol Nutr. 2008;47:493-9. [ ] 9. Liu KH, Chan YL, Chan WB, et al. Sonographic measurement of mesenteric fat thickness is a good correlate with cardiovascular risk factors: comparison with subcutaneous and preperitoneal fat thickness, magnetic resonance imaging and anthropometric indexes. Int J Obes Relat Metab Disord. 2003;27:1267-73. [ ] 10. Gong W, Ren H, Tong H, et al. A comparison of ultrasound and magnetic resonance imaging to assess visceral fat in the metabolic syndrome. Asia Pac J Clin Nutr. 2007;16 Suppl 1:339-45. [ ] 11. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19:231-40. [ ] 12. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307-10. [ ] 13. Sturm W, Sandhofer A, Engl J, et al. Influence of visceral obesity and liver fat on vascular structure and function in obese subjects. Obesity (Silver Spring). 2009;17:1783-8. [ ] 14. Ribeiro-Filho FF, Faria AN, Azjen S, et al. Methods of estimation of visceral fat: advantages of ultrasonography. Obes Res. 2003;11:1488-94. [ ] 15. Armellini F, Zamboni M, Rigo L, et al. The contribution of sonography to the measurement of intra-abdominal fat. J Clin Ultrasound. 1990;18:563-7. [ ] 16. Sabir N, Pakdemirli E, Sermez Y, et al. Sonographic assessment of changes in thickness of different abdominal fat layers in response to diet in obese women. J Clin Ultrasound. 2003;31:26-30. [ ] 17. Stolk RP, Wink O, Zelissen PM, et al. Validity and reproducibility of ultrasonography for the measurement of intra-abdominal adipose tissue. Int J Obes Relat Metab Disord. 2001;25:1346-51. [ ] 18. Tornaghi G, Raiteri R, Pozzato C, et al. Anthropometric or ultrasonic measurements in assessment of visceral fat? A comparative study. Int J Obes Relat Metab Disord. 1994;18:771-5. [ ] Received May 12, 2009. * Study developed at Unit of Ultrasonography, Hospital de Clínicas da Universidade Federal de Uberlândia (UFU), Uberlândia, MG, Brazil. |
|

{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554