Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 5 - Sep. / Oct. of 2009
Vol. 42 nº 5 - Sep. / Oct. of 2009
|
ICONOGRAPHIC ESSAY
|
|
Imaging findings of myocardial revascularization at multidetector computed tomography: where are the bypass grafts? An iconographic essay |
|
|
Autho(rs): Marcelo Targa Ripari, Rogério Santaniello, Roberto Sasdelli Neto, César Higa Nomura, Rodrigo Caruso Chate, Rodrigo Bastos Duarte Passos, Fernando Uliana Kay, Marcelo Buarque de Gusmão Funari |
|
|
Keywords: Multidetector coronary computed tomography angiography, Saphenous bypass graft, Coronary artery bypass graft |
|
|
Abstract:
IMDs, Radiologists, Fellows, Department of Imaging – Hospital Israelita Albert Einstein, São Paulo, SP, Brazil
INTRODUCTION Coronary artery disease (CAD) is one of the main causes of death in the world and surgical management by means of vascular bypass grafts is the technique of choice, particularly in cases of diffuse or multivascular disease. Annually, recurrence of symptoms of ischemia is observed in 4% to 8% of patients, and is closely related to the grafts patency(1,2). Currently, coronary cineangiography still remains as the gold standard in the postoperative follow-up of vascular bypass grafts. However, the assessment of patency of arterial and saphenous grafts utilized in the management of CAD has been performed by means of coronary computed tomography (CT) angiography since the introduction of multidetector CT equipment. Recently, a meta-analysis demonstrated the high accuracy of this method, with 98% sensitivity, 97% specificity, 93% positive predictive value, and 99% negative predictive value(3). Notwithstanding, one of the difficulties faced by the investigator during the analysis of chest images either focused on the evaluation of myocardial revascularization or not, is the identification and localization of the bypass graft course as well as the respective anastomoses that may vary among patients and according to the cardiac surgeon's experience and technique. The present essay includes a description of the main types of arterial grafts (right and left internal thoracic artery graft – RITA and LITA) and venous grafts (saphenous vein graft – SVG) through images reconstruction and coronary CT angiography images. The present iconographic essay is aimed at demonstrating the most frequent sites of arterial and venous bypass grafts for coronary arteries by reviewing coronary CT angiography studies performed in 64-row multidetector CT equipment in the postoperative follow-up of patients with previous history of myocardial revascularization. All the studies were performed in an Aquilion 64-row multidetector CT scanner (Toshiba Medical Systems; Tokyo, Japan) with ECG-gating and inspiratory breath-holding(4). The heart rate was previously controlled with beta-blocker, in accordance with the standard protocol of the institution. The images were acquired after 100–120 ml nonionic iodinated contrast (350 mg/ml) injection into antecubital vein at a rate of 5.0 ml/s. Later, the images were processed on a Vitrea workstation (Vital Images; Minnesota, USA), with multiplanar and 3D reconstructions.
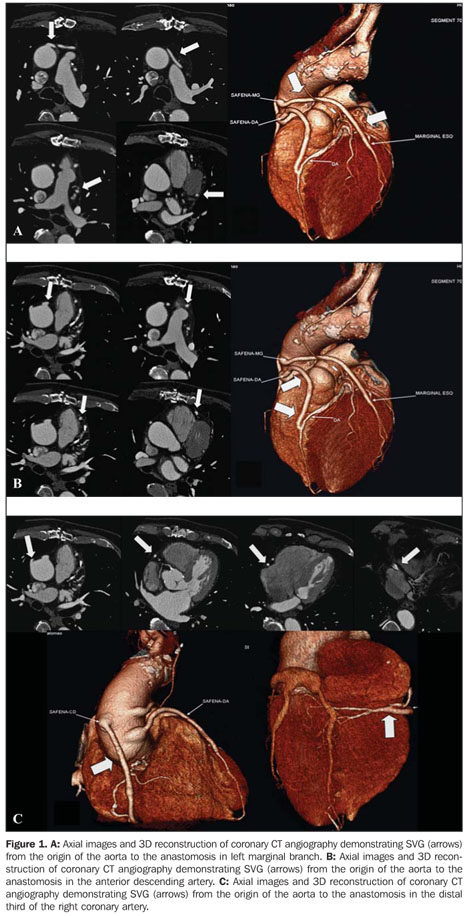
DESCRIPTION OF THE GRAFTS CAD can be surgically managed with either venous or arterial bypass grafts. Venous grafts Among the venous grafts, the most frequently utilized is the SVG, because of its availability, easy harvesting, favorable and widely utilized surgical technique(5) (Figure 1).
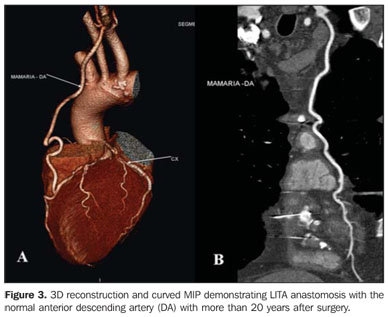
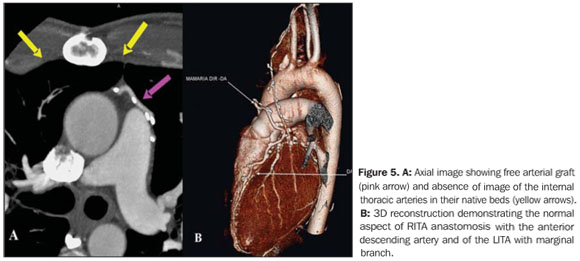
Arterial grafts Internal thoracic artery (ITA) – The LITA is most frequently utilized because of its anatomic proximity, surgical technique, improved survival and extent of the graft patency. Generally, the RITA requires more time to be displaced and anastomosed than the LITA does, and seems to be most frequently associated with mediastinal infection(5) (Figures 2, 3, 4 and 5).
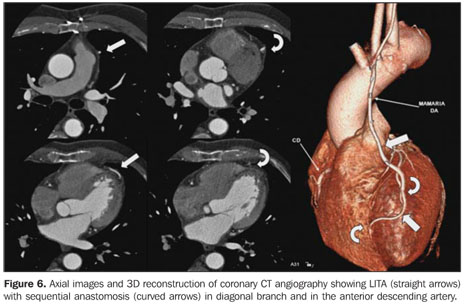
ITA grafts can be anastomosed with more than one vessel, with sequential, latero-lateral or latero-terminal techniques (Figure 6).
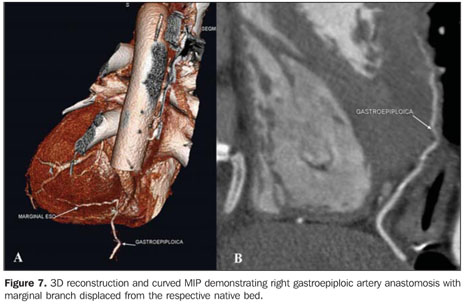
Radial artery – Some authors consider the radial artery graft as the second most relevant in myocardial revascularization. Thrombosis resulting from flow competition and spasm constitute complications that must be considered by the surgeon in the selection of the graft(5). Gastroepiploic artery – The right gastroepiploic artery is very useful as in situ graft combined with other grafts in procedures without extracorporeal circulation where clamping of aorta is not required (Figure 7). Limitations include: variable extent, vulnerability to flow competition and more extensive involvement of its origin by atherosclerosis, as compared with the ITA(5).
DISCUSSION Studies demonstrate rates of coronary artery graft occlusion ranging from 10% to 30% within 1 to 2 years, and from 45% to 55% within 10 to 12 years(6). Coronary cineangiography is the gold standard for demonstrating coronary artery grafts patency. However it is an invasive, highly expensive method that exposes the patients to some procedure-inherent risks such as acute myocardial infarct, cerebral vascular accident and ventricular arrhythmia, with estimated procedure-related mortality rate between 1% and 2%(7). Additionally, the absence of data regarding the grafts utilized in the patient interferes directly in the study, since the hemodynamicist will take more time, besides contrast agent and radiation exposure to search for and catheterizing the ITAs and SVGs. Coronary cineangiography and coronary CT angiography were compared by several studies, both for validating the new method in relation to the gold standard and for statistical comparison of the methods. This comparison demonstrates similar sensitivity and specificity in the visualization and characterization of grafts stenosis(5,7–9). In spite of the absence of data on the grafts utilized in the patient interfering in the analysis of the CT angiography study, it does not imply an increase in the radiation or contrast agent dose, affecting only the time required for the analysis of the images, since axial images provide all the mediastinal fields required for the search for grafts in a single acquisition. Thus, the localization of grafts and respective anastomoses on a study focused on coronary arteries and on general studies of the chest by computed tomography may represent a difficulty in the analysis of the images by a radiologist who is not familiar with the matter, since the knowledge on the surgical techniques utilized and the possible (usual and unusual) routes of the saphenous vein grafts and arterial anastomoses are useful in the analysis of both imaging methods, besides avoiding wrong diagnoses. The present iconographic essay also demonstrates some differences that allow the differentiation between arterial and venous grafts: arterial grafts generally present smaller caliber than venous grafts and frequently are associated with the presence of metal clips placed in the origin of their small branches. Venous grafts generally are calibrous and may present gross parietal calcifications associated with natural degeneration, besides fibrolipidic or "mixed" plaques(3,10). Therefore, the evaluation of the native bed of the internal thoracic arteries is relevant as a first step in this differentiation.
CONCLUSION Technical developments of CT equipment allow the identification of coronary artery and vein grafts on studies with and without ECG-gating so the knowledge on coronary grafts by radiologists is increasingly relevant.
REFERENCES 1. Cameron AAC, Davis KB, Rogers WJ. Recurrence of angina after coronary artery bypass surgery: predictors and prognosis (CASS registry). J Am Coll Cardiol. 1995;26:895–9. [ ] 2. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA guidelines for coronary artery bypass graft surgery. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1991 guidelines for coronary artery bypass graft surgery). J Am Coll Cardiol. 1999;34:1262–347. [ ] 3. Hamon M, Lepage O, Malagutti P, et al. Diagnostic performance of 16- and 64-section spiral CT for coronary artery bypass graft assessment: meta-analysis. Radiology. 2008;247:679–86. [ ] 4. Mahesh M, Cody DD. Physics of cardiac imaging with multiple-row detector CT. Radiographics. 2007;27:1495–509. [ ] 5. Frazier AA, Qureshi F, Read KM, et al. Coronary artery bypass grafts: assessment with multidetector CT in the early and late postoperative settings. Radiographics. 2005;25:881–96. [ ] 6. Ha JW, Cho SY, Shim WH, et al. Noninvasive evaluation of coronary artery bypass graft patency using three-dimensional angiography obtained with contrast-enhanced electron beam CT. AJR Am J Roentgenol. 1999;172:1055–9. [ ] 7. Yoo KJ, Choi D, Choi BW, et al. The comparison of the graft patency after coronary artery bypass grafting using coronary angiography and multi-slice computed tomography. Eur J Cardiothorac Surg. 2003;24:86–91. [ ] 8. Burgstahler C, Kuettner A, Kopp AF, et al. Non-invasive evaluation of coronary artery bypass grafts using multi-slice computed tomography: initial clinical experience. Int J Cardiol. 2003;90:275–80. [ ] 9. Ko YG, Choi DH, Jang YS, et al. Assessment of coronary artery bypass graft patency by multislice computed tomography. Yonsei Med J. 2003;44:438–44. [ ] 10. Feuchtner GM, Schachner T, Bonatti J, et al. Diagnostic performance of 64-slice computed tomography in evaluation of coronary artery bypass grafts. AJR Am J Roentgenol. 2007;189:574–80. [ ] Received June 29, 2009. Accepted after revision August 26, 2009. * Study developed at Department of Imaging – Hospital Israelita Albert Einstein, São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554