Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 3 - May / June of 2009
Vol. 42 nº 3 - May / June of 2009
|
ORIGINAL ARTICLE
|
|
Urethrovesical ultrasonography as an effective method for evaluating prognostic parameters in the surgical management of stress urinary incontinence |
|
|
Autho(rs): Frederico Teixeira Brandt, Risomar Belarmino Almeida, Arinaldo Vasconcelos de Alencar, Carla Daisy Costa Albuquerque, Agostinho de Sousa Machado Junior |
|
|
Keywords: Transvulvar ultrasonography, Perineal ultrasonography, Urethrovesical junction, Stress urinary incontinence, Burch surgery |
|
|
Abstract:
IPrivate Docent, Professor at Universidade Federal de Pernambuco (UFPE), Recife, PE, Brazil
INTRODUCTION Stress urinary incontinence is highly relevant not only as a disease, but principally due to the social repercussions and the consequences for the quality of patients' life.Because of the high prevalence of this condition, about 26 billion dollars are annually spent in the United States of America, with about 393.5 million being spent with diagnostic tests(1-3). The assumed diagnosis of stress urinary incontinence is eminently clinical. The most disseminated complementary study utilized for confirmation of the clinical hypothesis is the urodynamic study of the bladder and urethra that demonstrates the urinary loss in the absence of detrusor muscle contraction. However, the urodynamic study can only indirectly demonstrate the vertical mobility of the urethrovesical junction (UVJ) and proximal urethra (PU). Differently, ultrasonography can demonstrate a real image, with positioning and mobility of the UVJ and PU(4-20). Ultrasonography of the UVJ and PU has increasingly been used in the preoperative evaluation of patients with stress urinary incontinence as well as in their postoperative follow-up for defining topographic parameters regarding the UVJ and PU positioning according to the surgical technique utilized(4-13,17-19). An original study demonstrates that the UVJ and PU positioning represents a good prognostic factor of the success or failure of the surgical correction of stress urinary incontinence(14). The authors of the present study intend to utilize transvulvar ultrasonography for evaluating patients with stress urinary incontinence, analyzing the positioning and mobility of the UVJ and PU as a prognostic factor of Burch surgery.
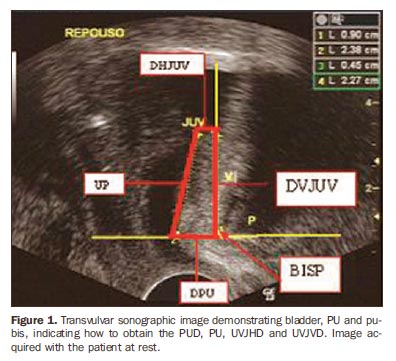
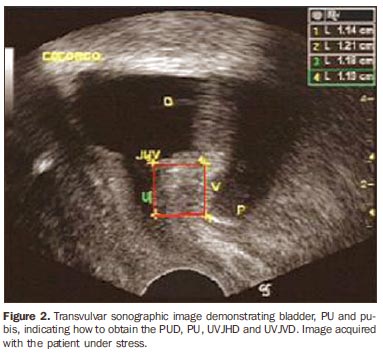
MATERIALS AND METHODS The project was approved by the Committee for Ethics in Research of the Center of Health Sciences of Universidade Federal de Pernambuco (UFPE). The present study included 30 women submitted to Burch surgery for stress urinary incontinence in the period from January/2005 to August/2007, who had attended the UFPE Unit of Research in Urinary Incontinence for postoperative evaluation. As regards the major stress urinary incontinence related complaint, 15 patients reported cure, and 15 returned with the same complaint that had motivated the surgery. Each of the patients included in the present study underwent ultrasonography up to 30 days before the surgery and also in the postoperative follow-up. Transvulvar ultrasonography studies of the UVJ and PU were performed in a SSD 500 Aloka equipment. The patient was placed in gynecological position, and a convex, 7 MHz transducer covered with a sterile condom was placed on the patient's vulva, between the outer lips, with the pressure necessary to acquire the images, but without any compression that could cause displacement of the structures under investigation. Images of the pubis, urethra, UVJ and bladder were acquired for measurement of the pubourethral distance (PUD), UVJ vertical distance (UVJVD), UVJ horizontal distance (UVJHD) and PU, at rest. The next step was asking the patient to exert a maximum abdominal effort downward (Valsalva maneuver), and the same measurements were performed. In the present study, PUD, UVJHD, UVJVD, PU, as well as variations in their displacement were evaluated. Sonographic variables are defined as follows: PUD - length in millimeters of a horizontal line from the inferior border of the pubic symphysis to the urethral portion crossed by this line. The intersection between the horizontal line and the urethral portion is called "urethral point"; PU - distance in millimeters between the UVJ and the urethral point, corresponding to the PU; UVJHD - length, in millimeters, of a horizontal line from the UVJ to the intersection with a vertical line originating from the inferior border of the pubic symphysis. Values at left of this line are positive, and at right, negative; UVJVD - length, in millimeters, of a vertical line, from the UVJ to the intersection with a horizontal line originating from the inferior border of the pubic symphysis. Values above this line are positive, and below, negative; Horizontal UVJ mobility - horizontal distance, in millimeters, corresponding to the UVJ displacement during stress (Valsalva maneuver), or the difference between the UVJHD at rest and the UVJHD under stress; Vertical UVJ mobility - vertical distance, in millimeters, corresponding to the UVJ displacement during stress (Valsalva maneuver), or the difference between the UVJVD at rest and the UVJVD under stress; PUD variation - corresponds to the difference between the PUD at rest and PUD under stress; PU variation - corresponds to the difference between the PU at rest and PU under stress. The sonographic parameters followed the concepts illustrated on Figures 1 and 2.
Combined Burch surgery was performed with a Pfannenstiel incision, and identification of the UVJ, urethra, pubocervical fascia of the inferior third of the vagina and vesicovaginal junction in the Retzius space. Two points of prolene 0 suture were applied on the right paraurethral fascia, at 2 cm and 4 cm from the urethra, and at 1 cm from the vesical base. The same points were applied on the left side of the urethra. Bilateral transfixion of the Cooper ligaments by the suture, kept them in parallel to each other, and moderately fastened to elevate the paraurethral fascia and the UVJ. The continuous variables results were expressed as means ± standard deviations. Each of the variables evaluated in the different groups was submitted to variance analysis. The Fisher's exact test was utilized for comparing group 1 and group 2 results. A 95% confidence interval was accepted, and p < 0.05 was considered as significance level.
RESULTS The results are demonstrated on Tables 1, 2, 3 and 4, as follows.
Table 1 - Click here to enlarge
Table 2 - Click here to enlarge
Table 1 - Click here to enlarge
Table 4 - Click here to enlarge
The PUD at rest and under stress presented no significant variation (p > 0.05) between groups 1 and 2 in the preoperative and postoperative periods (Table 1). The UVJHD presented no significant variation (p > 0.05) between groups 1 and 2, at rest, under stress and displacement, in the preoperative and postoperative periods (Table 2). In group 2, the UVJVD was significantly shorter under stress, in the postoperative period, and the UVJ displacement was significantly larger (Table 3). The PU variable presented a significant difference (p < 0.05) between groups 1 and 2 for displacement, both in the pre- and postoperative periods, and under stress in the postoperative period (p < 0.01). The lower standard deviations were observed with displacement, in the postoperative period, group 1 (2.90 mm) and preoperative period, group 2 (3.52 mm) (Table 4).
DISCUSSION In the present study, the main objective was testing the hypothesis already published in the literature, that the investigation of UVJ and PU by transvulvar ultrasonography can be utilized for evaluating the prognosis of the surgical management of stress urinary incontinence(14). The great differential in the present research is a novel demonstration that the prognostic factor can be early detected in the preoperative period through a shorter PU displacement in women affected by recidivation of stress urinary incontinence. However, the results of the present study must be confirmed by other researchers. It is the authors' intention to further investigate the same hypothesis with other surgical techniques for management of stress urinary incontinence. In order to answer a proposed question, the Burch surgery was utilized because this technique can be considered as a golden standard(18) in the management of stress urinary incontinence and has been performed as a standard in the UFPE Unit for Research in Urinary Incontinence for more than ten years. However, until the contrary is proved by the argument that the surgical treatment must achieve the UVJ and PU repositioning in compliance with the logics of the passive urinary continence, what is valid for Burch surgery must correspond to other surgical procedure(15). Based on the concept of passive urinary continence, the surgical management of stress urinary incontinence consists in permanently recover the vertical UVJ mobility and the PU distance(16). As a matter of fact, in the present study, among the cured patients, only one of them (6.7%) presented hypermobility in the postoperative follow-up, while among the non-cured patients this rate increased to 53.4%. Although the present study has been developed with women submitted to Burch surgery for management of stress urinary incontinence, it is theoretically possible to extrapolate that the same anatomophysiological behavior should be observed with any other technique for management of stress urinary incontinence. Thus, pre- and postoperative sonographic evaluation of UVJ and PU must be appropriately performed in patients treated for stress urinary incontinence by means of other surgical procedure for determining prognostic factors for cure and non-cure. The actual relevance of the horizontal positioning of the UVJ and PU in the pre-and postoperative investigation of stress urinary incontinence is still to be determined. Most probably, there must be some correlation that still remains undefined. But it is possible to affirm that there is a correlation between these sonographic parameters statically and dynamically evaluated with the success and failure of the surgical management of women with stress urinary incontinence.
CONCLUSION Ultrasonography of the UVJ and PU can be considered as an effective method for evaluating prognostic parameters for the surgical management of women with stress urinary incontinence.
REFERENCES 1. Fultz N, Girts T, Kinchen K, et al. Prevalence, management and impact of urinary incontinence in the workplace. Occup Med (Lond). 2005;55: 552-7. [ ] 2. Weber AM, Taylor RJ, Wei JT, et al. The cost-effectiveness of preoperative testing (basic office assessment versus urodynamics) for stress urinary incontinence in women. BJU Int. 2002;89:356-63. [ ] 3. Kocak I, Okyay P, Dundar M, et al. Female urinary incontinence in the west of Turkey: prevalence, risk factors and impact on quality of life. Eur Urol. 2005;48:634-41. [ ] 4. Brandt FT, Albuquerque CDC, Lorenzato FR, et al. Perineal assessment of urethrovesical junction mobility in young continent females. Int Urogynecol J Pelvic Floor Dysfunct. 2000;11:18-22. [ ] 5. Brandt FT, Oliveira RR, Albuquerque CDC, et al. Incontinência urinária de urgência no contexto da incontinência urinária de esforço. J Bras Ginecol. 1998;98:183-4. [ ] 6. Brandt FT, Albuquerque CDC, Arraes AF, et al. Influência do volume vesical na avaliação ultrasonográfica da junção uretrovesical e uretra proximal. Radiol Bras. 2005;38:33-6. [ ] 7. Tunn R, Petri E. Introital and transvaginal ultrasound as the main tool in the assessment of urogenital and pelvic floor dysfunction: an imaging panel and practical approach. Ultrasound Obstet Gynecol. 2003;22:205-13. [ ] 8. Brandt FT, Nóbrega LV, Albuquerque CDC, et al. Aferição simultânea da pressão abdominal na avaliação ultra-sonográfica de mulheres com incontinência urinária de esforço. Radiol Bras. 2006;39:91-5. [ ] 9. Brandt FT, Santos Junior MW, Albuquerque CDC, et al. Modificações da junção uretrovesical e uretra proximal após a cirurgia de alça sem tensão em mulheres de 45 a 72 anos. Rev Bras Saude Mater Infant. 2005;5:185-91. [ ] 10. Dalpiaz O, Curti P. Role of perineal ultrasound in the evaluation of urinary stress incontinence and pelvic organ prolapse: a systematic review. Neurourol Urodyn. 2006;25:301-6. [ ] 11. Sendag F, Vidinli H, Kazandi M, et al. Role of perineal sonography in the evaluation of patients with stress urinary incontinence. Aust N Z J Obstet Gynaecol. 2003;43:54-7. [ ] 12. Weidner AC, Myers ER, Visco AG, et al. Which women with stress incontinence require urodynamic evaluation? Am J Obstet Gynecol. 2001; 184:20-7. [ ] 13. Kil PJ, Hoekstra JW, van der Meijden AP, et al. Transvaginal ultrasonography and urodynamic evaluation after suspension operations: comparison among the Gittes, Stamey and Burch suspensions. J Urol. 1991;146:132-6. [ ] 14. Viereck V, Pauer HU, Hesse O. Urethral hypermobility after anti-incontinence surgery - a prognostic indicator? Int Urogynecol J Pelvic Floor Dysfunct. 2006;17:586-92. [ ] 15. Ribeiro CBL, Brandt FT, Albuquerque CD, et al. Modificações da uretra proximal e da junção uretrovesical, decorrentes da cirurgia do tipo Kelly-Kennedy. Acta Cir Bras. 2001;17:21-3. [ ] 16. Brandt FT. Importância da junção uretrovesical na continência urinária passiva e na incontinência urinária de esforço. J Bras Ginecol. 1996;106: 259-62. [ ] 17. Brandt FT, Albuquerque CDC, Lorenzato FRB, et al. A importância da ultra-sonografia transvulvar na avaliação de parâmetros anatômicos relevantes no tratamento de mulheres com incontinência urinária de esforço. Radiol Bras. 2007;40: 371-6. [ ] 18. Martan A, Masata J, Halaska M, et al. Ultrasound imaging of the lower urinary system in women after Burch colposuspension. Ultrasound Obstet Gynecol. 2001;17:58-64. [ ] 19. Chene G, Cotte B, Tardieu AS, et al. Clinical and ultrasonographic correlations following three surgical anti-incontinence procedures (TOT, TVT and TVT-O). Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:1125-31. [ ] 20. Brandt FT, Lorenzato F, Albuquerque CDC, et al. Tension-free vaginal tape versus lata fascia sling: the importance of transvulvar ultrasound in the assessment of relevant anatomical parameters in treatment of women with stress urinary incontinence. Indian J Urol. 2009;25:62-7. [ ]
Received November 22, 2008.
* Study developed at the Unit for Research in Urinary Inconti-4. MD, Resident of Gynecology & Obstetrics, Substitute Pronence - Universidade Federal de Pernambuco (UFPE), Recife, PE, fessor of Obstetrics, Universidade Federal de Pernambuco (UFPE), Brazil. Recife, PE, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554