Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 3 - May / June of 2009
Vol. 42 nº 3 - May / June of 2009
|
ORIGINAL ARTICLE
|
|
Uncommon presentations of intraosseous hemophilic pseudotumor in imaging diagnosis |
|
|
Autho(rs): Marcel Koenigkam Santos, Mariana Basso Polezi, Edgard Eduard Engel, Mônica Tempest Pastorello, Marcelo Novelino Simão, Jorge Elias Junior, Marcello Henrique Nogueira-Barbosa |
|
|
Keywords: Magnetic resonance imaging, Pseudotumor, Hemophilia |
|
|
Abstract:
IPhD, Radiologist, Assistant at Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRP-USP), Ribeirão Preto, SP, Brazil
INTRODUCTION Hemophilia is a blood coagulation disorder characterized by low factors VIII or IX activity corresponding respectively to types A and B. Hemophilia A, or the classical presentation of the disease, is more common, with a prevalence of 1:10,000, while hemophilia B or "Christmas disease" is found in 1:50,000 to 1:100,000 individuals. Both types of hemophilia originate in X-linked recessive genetic inheritance carried by women and manifested in men. Clinical and radiological signs of both types of hemophilia are similar. Repeated bleedings with formation of hematomas and hemarthrosis are the most frequent musculoskeletal manifestations of the disease. Muscles most commonly involved include the iliopsoas and the gastrocnemius. In decreasing order, the joints most frequently affected are: knee, ankle, elbow, shoulder and hip, with the resulting chronic joint disease being called hemophilic arthropathy(1). Pseudotumor is a rare complication, occurring in only 1% to 2% of hemophilic patients, independently from type A or B, however is more frequently found in adults with severe hemophilia (patients with levels of < 1% of coagulation factor)(2). The development of a pseudotumor results from chronic and recurrent hemorrhages that lead to the formation of an encapsulated mass containing blood at different stages of degradation. Eventually, the hemophilic pseudotumor may progress to a very large lesion. The pseudotumor may develop in soft tissues, or may be intraosseous or subperiosteal, in this decreasing order of frequency(3). In the present study, imaging findings of five lesions from intraosseous hemophilic pseudotumors in two patients are presented, highlighting presentations that are not frequently found in literature reports. One of them is the apparently solid, heterogeneous post-contrast enhancement within a pseudotumor. The post-contrast enhancement has been better documented on computed tomography (CT) images, considering that, at magnetic resonance imaging (MRI), such areas already presented a strong spontaneous hyperintense signal on the precontrast, T1-weighted sequences, because of hemoglobin degradation products. In this same femoral pseudo-tumor, an extension by contiguity of the lesion to the posterior tibial region was observed, which is also an uncommon finding. Another uncommon presentation described in the present study corresponds to the presence of two lesions in a same long bone, the humerus, with an interposition of o segment of healthy bone between both lesions.
MATERIALS AND METHODS Plain radiographs, CT and MRI images of two hemophilic patients were consensually reviewed by two musculoskeletal radiologists with at least a 10-year experience in this subspecialty. Both patients were white and had been diagnosed with hemophilia type A, one of them severely affected and the other, moderately affected by the disease (1% to 5% of coagulation factor). The radiographs were made in conventional equipment. The CT images were acquired in helical equipment, with axial sections of the limbs and 15 mm-thick slices, before and after intravenous contrast injection, with bone and soft tissue windows. MRI images were acquired with different sequences in the three planes with a 1.5 T closed field superconductor equipment, and appropriate coils. Intravenous paramagnetic contrast was utilized in both the patients. The patient with moderate hemophilia (patient 1) was 22 years old and presented two lesions affecting the right thigh and arm. The diagnosis of hemophilia had been confirmed at four years of age, following investigation for repeated hemorrhages, mainly in the gingival. This patient has a history of trauma in the region previously to the manifestation of pseudotumors, with reports on clinical records of diaphyseal fracture of the humerus and femur. The radiographs from the time of the trauma were not found. The lesion diagnosis was confirmed by anatomopathological study, after suprapatellar amputation of the right lower limb and supracondylar amputation of the right upper limb, both surgeries indicated because of infection of the lesions with no response to the clinical treatment. The patient with severe hemophilia (patient 2) was 20 years old and presented three lesions, also in the right thigh and arm. During the investigation of muscular hematomas at the first year of life, the diagnosis of hemophilia had already been confirmed. The history of trauma in the regions where the pseudotumors developed was also reported on the patient's clinical records. In the case of this patient, anatomopathological confirmation was obtained after amputation of the right upper limb and resection of the femoral diaphysis with bone endoprosthesis implantation. Both surgeries were indicated for compartment syndrome and pain unresponsive to treatment.
RESULTS On the patients 2 radiographic images, two lytic expansile lesions with marginal sclerosis and bone cortical thinning and discontinuity were observed. On the other hand, in the case of patient 1, the lesions presented a more aggressive appearance, with volume and density increase in the soft parts of the limb, regions with bone resorption and fragmentation of the involved bone (Figure 1).
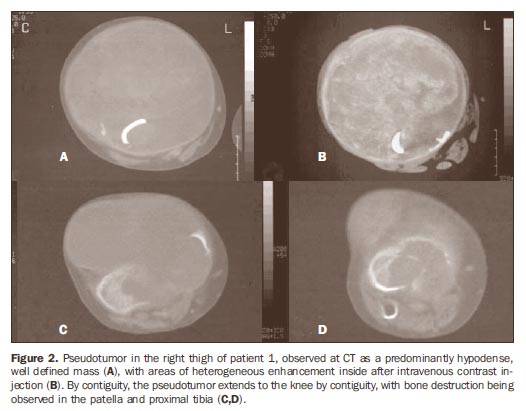
At CT, the lesions were characterized as well defined masses and heterogeneous contents, with predominant hypoattenuating areas associated with expansion and destruction of the affected bones. In the patient 1, the post-contrast phase demonstrated irregular areas of heterogeneous enhancement within on the right thigh (Figure 2).
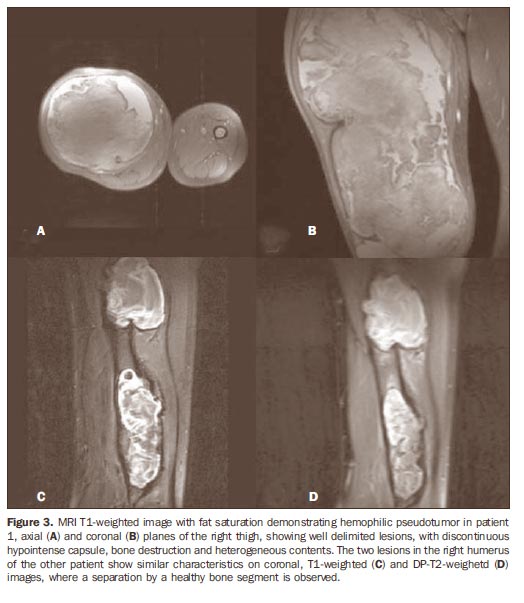
Both patients underwent MRI. In the patient 1, only the lesion of the right femur was studied, as the amputation of the right upper limb had already been performed. In this patient, considerable enlargement of the lower limb was observed with an expansile, well defined lesion, measuring 41.0 × 21.0 × 15.0 cm, and irregular and discontinuous capsule with hypointense signal on all the sequences. The lesion content was heterogeneous, with predominant areas of hyperintense signal on T1- and T2weighted sequences. Foci of low signal intensity were also observed, correlating with the presence of bone fragments and hemosiderin (Figure 3). The lesion presented a subtle heterogeneous enhancement after paramagnetic contrast injection, considerably less evident than the one observed at CT. In the femoral lesion of the patient 1, the extension of the femoral lesion to the bones of the knee joint was identified, with bone destruction in the patella and in the posterior aspect of the tibia.
In the patient 2, three lesions were evaluated by MRI. A dyaphyseal segment of healthy bone was observed separating the two lesions in the right humerus. The signal intensity characteristics of these two lesions were similar to those in the third lesion of the right femur of the same patient. The humeral pseudotumors measured 9.0 and 8.0 cm in their largest diameter, while the femoral lesion reached 15.0 cm in its largest diameter. At MRI, the heterogeneous contents of the lesions could be clearly observed, with areas of hypointense signal on T1- and T2-weighted sequences. The femoral lesion was exclusively intraosseous, with cortical bulging, while the lesions in the humerus presented areas with discontinuous bone cortical, with components of soft tissue and an irregular hypointense halo on all the sequences. In this patient, no pathological enhancement was observed after paramagnetic contrast injection.
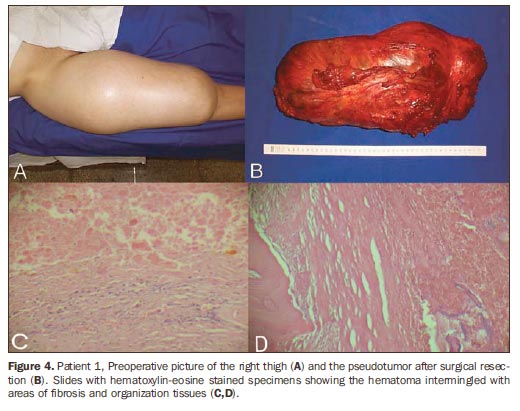
DISCUSSION The present study describes two patients with a total of five intraosseous hemophilic pseudotumors (two in the femur, and three in the humerus) evaluated by plain radiography, CT and MRI. According to the literature, femur, hip, tibia and the hand bones are most frequently affected(4). Pseudotumor was first described in 1918 by Starker et al.(5), and at that time the expansile character of this lesion was highlighted, as an indication of the differential diagnosis with malignant neoplasm. At radiography, bone hemophilic pseudotumors are seen as osteolytic, well defined expansile, uni- or multilocular lesions. Eventually the lesions show endosteal scalloping, thickening, thinning or even discontinuity of the bone cortical. Marginal sclerosis and dystrophic calcifications may occur. The presence of discontinuous periosteal reaction, which is frequently present in malignant bone lesions, has been described in cases of bone hemophilic pseudotumor(6). In 1972, Brant & Jordan(6) thoroughly reviewed the radiographic findings of pseudotumor, and emphasized the relevance of acute trauma, even when small, related to the hemorrhage that originates the initial lesion. Depending on the number and extent of the subsequent bleedings, this lesion leads to the formation of the pseudotumor that may develop in a matter of weeks or even years. In the case of the two patients included in the present study, the history of trauma in the sites of the pseudotumor was registered on their clinical records. At CT, the hemophilic pseudotumor is generally visualized as a lesion with multicystic aspect, with well defined limits and eventually with more marked bone destruction. At the acute phase, the center of the lesion is hypodense, and the peripheral area presents an attenuation coefficient similar to one of the adjacent musculature. Like in other hemorrhagic lesions, fluid levels are frequently found at images of sectional imaging methods. After intravenous contrast injection, a peripheral enhancement is most frequently observed, with the outlining of the pseudocapsule of the lesion(7). The presence of heterogeneous enhancement in neoplastic masses is caused mainly by neoangiogenesis, with the formation of pathological vessels, with altered resistance and permeability(8). In one of the lesions described in the present study, enhancement was observed after intravenous contrast injection, which might have deviated the rationale in the differential diagnosis, in case the radiologist were not aware of the clinical information. Because of bleedings in different times, the hemophilic pseudotumor may present irregular septations and even solid areas of organization, with fibrocicatricial tissue that may present enhancement after intravenous contrast injection(9). The radiologist and the assisting physician must have knowledge of these presentations, albeit uncommon, in order to perform an appropriate evaluation and avoiding unnecessary biopsy, obviously undesirable in a hemophilic patient, because of the high incidence of complications, including bleedings, fistula and infection(10). The heterogeneous aspect of the lesion contents at MRI is caused by the different stages of bleeding and blood degradation. The more peripheral areas with hypointense signal on T1-weighted images correspond to fluid with intra- and extracellular meta-hemoglobin, i.e. degrading blood, in a period from three days to four weeks. The most central portions of the lesion where intermediate to hypointense signal predominates, correspond preferably to the presence of deoxyhemoglobin originated from extravasation of red blood cells in the previous 24 to 72 hours. The center of the lesion tends to become heterogeneously hyperintense with the progress of the hemoglobin degradation. The hypointense capsule that may outline the hemophilic pseudotumor, specially the muscular ones, is formed by fibrotic tissue, with hemosiderin contained in the macrophages, aspects that justify the low signal intensity observed on T1- and T2-weighted sequences. The halo is more easily identified on T2weighted, fast spin echo and gradient echo sequences(3,7,9,11,12). The characteristics of the lesions observed at MRI were confirmed by anatomopathological study. Such studies demonstrated extensive hematomas at several stages of development, with areas of organization and fibrosis, presence of histiocytes containing hemosiderin, mainly in the regions where a firm and chestnut-shaped capsule is observed involving the lesion (Figure 4).
Jaovisidha et al.(11), reviewing the spectrum of MRI findings of hemophilic pseudo-tumors, have described the presence of peripheral solid nodules, particularly in muscular lesions, corresponding to small hematomas resulting from the rupture of small adjacent muscular vessels. In such lesions, the presence of smaller cystic lesions, or "subsidiary cysts", can be observed and, according to the authors, it should be reported for an appropriate surgical planning. The present study describes the case of a patient with severe hemophilia who presented two intraosseous pseudotumors separated by a segment of healthy bone, a different presentation with no similar report in the literature. MRI was the method that better demonstrated this presentation, probably secondary to traumas at different times on the same bone. In the other patient, with moderate hemophilia, the authors describe a large pseudotumor with a more aggressive solid aspect, and heterogeneous contrast enhancement at CT, resembling the aspect of a malignant neoplasm. The grading of hemophilia is based on the rate of coagulation factor, and a single patient may be reclassified with the progression and treatment of the disease. Patients with severe disease may present spontaneous bleedings, but even those with moderate or mild hemophilia may disproportionally present major bleedings following minor traumas(1). Therefore, the presence of a more aggressive lesion in a patient with moderate disease should not be interpreted as unexpected or incompatible. The differential diagnosis for hemophilic pseudotumor may be reached with several benign, malignant or even infectious lesions, especially when presenting intra tumor hemorrhage. At imaging diagnosis, intraosseous hemophilic pseudotumors may simulate several lesions such as giant cell tumors, desmoplastic fibroma, plasmocytoma, metastasis, Ewing's sarcoma, osteosarcoma, aneurysmal bone cyst, brown tumor of hyperparathyroidism and hydatid disease(8,13). Although several lesions may present imaging findings similar to those of hemophilic pseudotumors, this difficulty is normally overcome by the knowledge of the patient's clinical history. The imaging findings, however, may be specific enough to significantly restrict the differential diagnosis, by demonstrating the capsule of the lesion and the contents with hemoglobin degradation products at different stages(14). If the pseudotumor is rapidly diagnosed, while the lesion is still small, the clinical management, which includes bone replacement therapy and immobilization, may be resolutive. However, in cases where lesion becomes extensive, sometimes involving neurovascular structures, surgery may become the only viable option. Many times, the only surgical option is a mutilating alternative, with amputation of the limb in volved(15,16). MRI may play a significant role in the follow up of pseudotumor progression, particularly in the differentiation between recent bleedings and previous and organized bleedings.
REFERENCES 1. Resnick D, Kransdorf MJ. Bone and joint imaging. 3rd ed. Philadelphia: Elsevier Saunders; 1995. [ ] 2. Ahlberg AK. On the natural history of hemophilic pseudotumor. J Bone Joint Surg Am. 1975;57: 1133-6. [ ] 3. Wilson DA, Prince JR. MR imaging of hemophilic pseudotumors. AJR Am J Roentgenol. 1988;150:349-50. [ ] 4. Kerr R. Imaging of musculoskeletal complications of hemophilia. Semin Musculoskelet Radiol. 2003;7:127-36. [ ] 5. Starker L. Knochenusur durch ein hamophiles, subperiostales Hamatom. Mitt Med Chir. 19181919;31:381. [ ] 6. Brant EE, Jordan HH. Radiologic aspects of hemophilic pseudotumors in bone. Am J Roentgenol Radium Ther Nucl Med. 1972;115:525-39. [ ] 7. Hermann G, Gilbert MS, Abdelwahab F. Hemophilia: evaluation of musculoskeletal involvement with CT, sonography, and MR imaging. AJR Am J Roentgenol. 1992;158:119-23. [ ] 8. Fechner RE, Mills SE. Atlas of tumor pathology: tumors of the bone and joints. 3rd ed. Washington, DC: Armed Forces Institute of Pathology; 1993. [ ] 9. Geyskens W, Vanhoenacker FM, Van der Zijden T, et al. MR imaging of intra-osseous hemophilic pseudotumor: case report and review of the literature. JBR-BTR. 2004;87:289-93. [ ] 10. Magallón M, Monteagudo J, Altisent C, et al. Hemophilic pseudotumor: multicenter experience over a 25-year period. Am J Hematol. 1994; 45:103-8. [ ] 11. Jaovisidha S, Ryu KN, Hodler J, et al. Hemophilic pseudotumor: spectrum of MR findings. Skeletal Radiol. 1997;26:468-74. [ ] 12. Park JS, Ryu KN. Hemophilic pseudotumor involving the musculoskeletal system: spectrum of radiologic findings. AJR Am J Roentgenol. 2004; 183:55-61. [ ] 13. Stafford JM, James TT, Allen AM, et al. Hemophilic pseudotumor: radiologic-pathologic correlation. Radiographics. 2003;23:852-6. [ ] 14. Ng WH, Chu WC, Shing MK, et al. Role of imaging in management of hemophilic patients. AJR Am J Roentgenol. 2005;184:1619-23. [ ] 15. Hermann G, Yeh HC, Gilbert MS. Computed tomography and ultrasonography of the hemophilic pseudotumor and their use in surgical planning. Skeletal Radiol. 1986;15:123-8. [ ] 16. Gaary E, Gorlin JB, Jaramillo D. Pseudotumor and arthropathy in the knees of a hemophiliac. Skeletal Radiol. 1996;25:85-7. [ ] Received January 7, 2009. * Study developed at Centro de Ciências das Imagens e Física Médica do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (CCIFM/HCFMRPUSP), Ribeirão Preto, SP, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554