Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 3 - May / June of 2010
Vol. 43 nº 3 - May / June of 2010
|
ICONOGRAPHIC ESSAY
|
|
Brain 18F-FDG PET-MRI coregistration: iconographic essay |
|
|
Autho(rs): José Leite Gondim Cavalcanti Filho, Léa Mirian Barbosa da Fonseca, Romeu Côrtes Domingues, Roberto Côrtes Domingues, Luiz Souza de Machado Neto, Emerson Leandro Gasparetto |
|
|
Keywords: Fluorodeoxyglucose, FDG, Positron emission tomography, PET, Magnetic resonance imaging, Fusion, Clinical neurology |
|
|
Abstract:
INuclear Physician at Clínica Multi-Imagem PET, Rio de Janeiro, RJ, Brazil
INTRODUCTION Recent clinical studies have demonstrated that combined positron emission tomography/computed tomography (PET/CT) offers higher accuracy in the evaluation of patients with suspicion of malignancy and disease staging than other methods where the study is made through interpretation of PET or CT images alone(1). In clinical practice, the use of multimodality imaging methods has already become a reality, particularly in the field of nuclear medicine, and practically the whole range of PET equipment, actually, represents integrated PET and CT systems. The interpretation of PET images alone without fusion with other imaging modalities with a better anatomical definition such as CT or magnetic resonance imaging (MRI), presents a low specificity and decreased positive predictive value. In the last few years, a lot has been researched on PET/MRI coregistration(2). A high potential is estimated for these methods integration in the diagnosis of neurological diseases, because PET is highly sensitive for detecting metabolic changes, but presents a limited spatial resolution. On the other hand, MRI presents a high spatial resolution in the evaluation of structures with soft tissues signal such as the brain, additionally to the functional capability of the method.
TECHNICAL ASPECTS Basically, there are three systems for integrating PET and MRI(3), as follows: 1) independent PET and MRI apparatuses in separate rooms. The images coregistration is performed with dedicated softwares, which generates flexibility, considering that both methods can be separately utilized; 2) sequential images acquired in different apparatuses, but the patient remains on a single examination table that is used on both the systems. Therefore, this is a hardware-fused system; 3) a completely integrated systems where the images are simultaneously acquired, for example, with a single examination table positioning, neither the patient nor the table is moved in the process of images acquisition. In some cases, simultaneous images acquisition is essential, considering that certain radiopharmaceuticals present a different pharmacokinetics. For example, H2O-15O passes through the region of interest in a matter of minutes, thus in this case this type of acquisition is required. On the other hand, fluorodeoxyglucose (FDG) takes about 45 minutes to be biodistributed, so simultaneous images acquisition is not relevant in this case. Images fusion was already utilized even before the introduction of hybrid systems. In fact, it was this method that paved the way to images coregistration by hybrid systems. Brain images coregistration with software is already validated because of the static nature of this organ(4). A comparison of several softwares available for MRI and PET/CT fusion, demonstrated a 2-3 mm accuracy that is smaller than the size of one PET pixel(4). Thus, the fusion of brain FDG-PET images and MRI becomes an attractive method for noninvasive evaluation of neurological diseases.
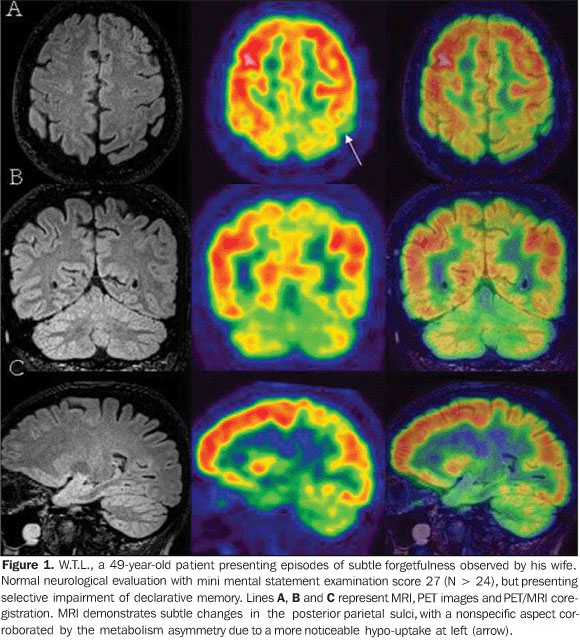
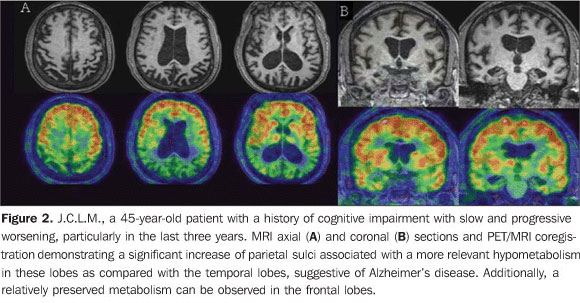
PET/MRI COREGISTRATION IN COGNITIVE IMPAIRMENT/DEMENTIA Recently, the concept of mild cognitive impairment (MCI) was introduced to describe a memory deficit similar to, but without other criteria of Alzheimer's disease(5). Patients with mild cognitive impairment present a rate of conversion to Alzheimer's disease of approximately 10-15% per year. For this reason, the recognition of such patients is important so that a treatment can be defined as the earliest as possible. About 60-70% of patients with mild cognitive impairment and presenting mild to severe association cortex hypometabolism (Figure 1), even with a mini mental statement examination (MMSE) scored as normal, may progress to dementia within two years. Early Alzheimer's disease tends to present hypometabolism in the parietal, temporal lobes and posterior cingulate cortex. This change can be easily identified at FDG-PET (Figure 2)(6).
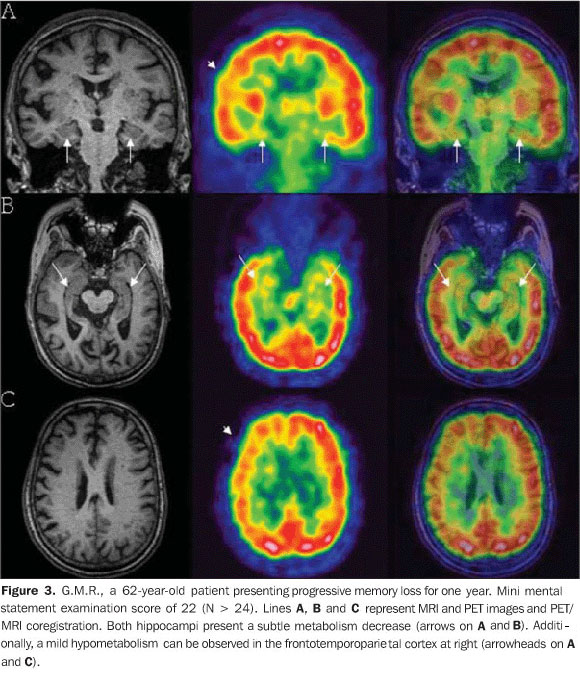
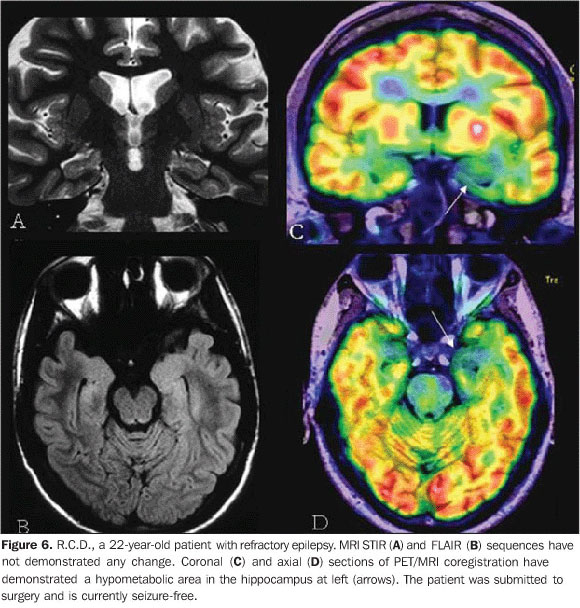
The relevance of the fusion of FDG-PET images and MRI is associated with the identification of metabolic changes in small-sized structures that are difficult to be anatomically localized at PET, such as the hippocampus, for example (Figure 3), that is intimately related to a future cognitive impairment and Alzheimer's disease, as well as the angular gyrus and the precuneus.
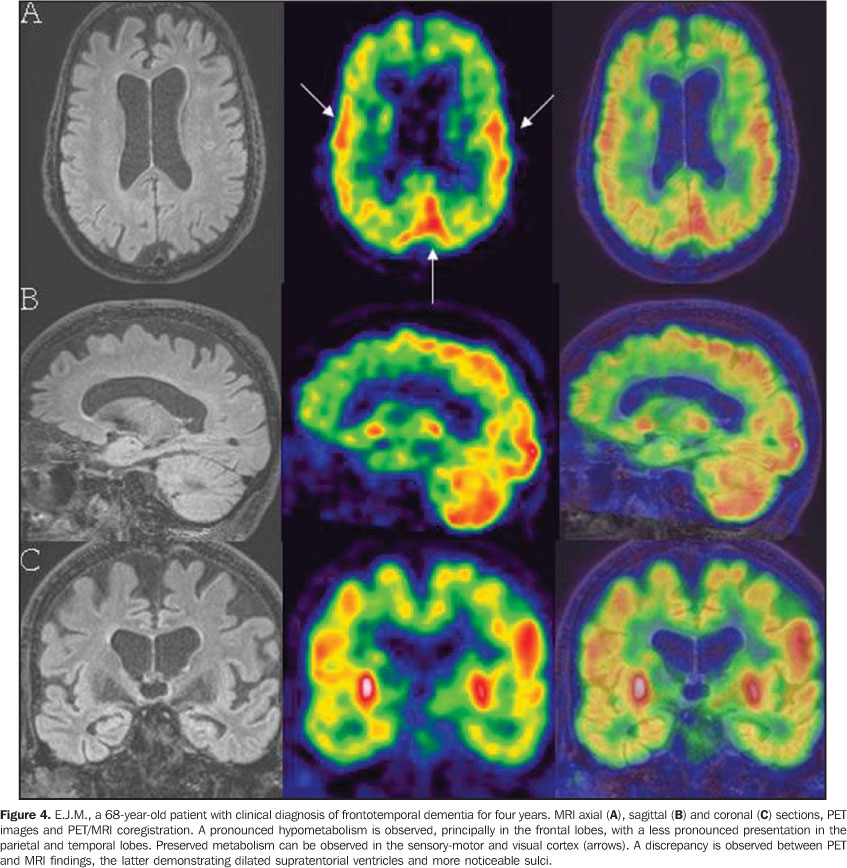
Frontotemporal dementia is not a specific clinical entity, comprising a spectrum including from a classic Pick's disease to a primary progressive aphasia. It can be identified with PET in the presence of either frontal or frontotemporal hypometabolism (Figure 4). The clinical diagnosis of vascular dementia represents a diagnostic challenge, since a consensus is still to be reached and the convergence among specialists is poor. Additionally, about 20-40% of patients vascular dementia is associated with Alzheimer's disease(7). Considering that MRI is highly sensitive in the evaluation of structural lesions, but poorly specific for Alzheimer's disease, the diagnosis of vascular dementia is frequently tendentious. For this reason, the fusion of metabolic PET images with structural MRI emerges as a relevant tool in the correct classification of these dementias.
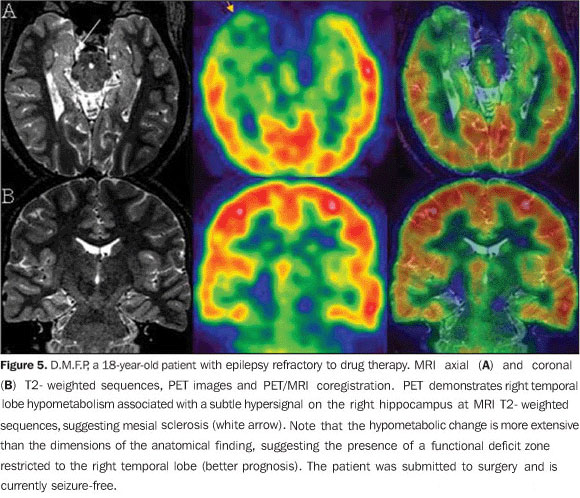
PET/MRI COREGISTRATION IN EPILEPSY The drug therapy for epilepsy is ineffective in a considerable number of patients. Complete resection of the epileptogenic focus may prevent future seizures in 90% of patients with mesial temporal lobe epilepsy, and in up to 70% of patients with cortical dysplasia. MRI is the method of choice in the investigation of epileptogenic lesions. FDG-PET adds relevant prognostic information, since it is known that hypometabolism restricted to the temporal lobe is correlated with surgical healing in 75% of these patients, as compared with only 45% of patients with extratemporal hypometabolism (Figures 5 and 6)(8).
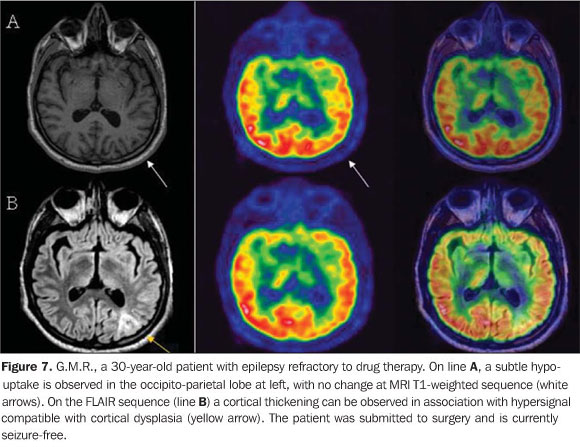
A relevant role is played by FDG-PET/MRI coregistration in the identification of cortical dysplasia (Figure 7), particularly in patients with Palmini type 1 focal cortical dysplasia, leading to an increase of 18% in the detection of this disease(9).
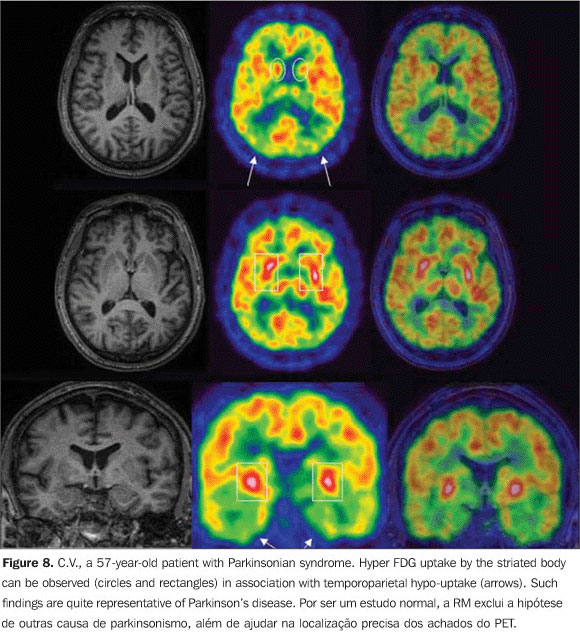
PET/MRI COREGISTRATION IN PARKINSONISM Clinically differentiating among parkinsonian syndromes may be very difficult. Morphological studies such as CT and MRI are usually used to rule out other causes that may be leading to parkinsonism. FDG-PET may be utilized in dubious cases (Figure 8)(10).
Besides the already described Parkinson's disease, other types of parkinsonism such as progressive supranuclear palsy, multiple system atrophy and corticobasal degeneration may be investigated. Radiotracers such as FDOPA-18F and 11C-Raclopride are more specific since they can indicate the function and integrity of pre- and postsynaptic dopaminergic terminals. However, these radiopharmaceuticals are not available yet to the Brazilian market.
CONCLUSION Considering that the fusion of brain images with software is highly accurate, the most sensitive and specific modality for detection of metabolic changes (PET) can be associated with other modality with high spatial resolution, besides evaluating structures with soft tissues signal intensity with excellent contrast resolution (MRI). Therefore, brain PET/MRI coregistration becomes an extremely attractive noninvasive method for evaluating neurological diseases.
REFERENCES 1. Ishikita T, Oriuchi N, Higuchi T, et al. Additional value of integrated PET/CT over PET alone in the initial staging and follow up of head and neck malignancy. Ann Nucl Med. 2010 Jan 8. [Epub ahead of print] [ ]. 2. Yamamoto S, Imaizumi M, Kanai Y, et al. Design and performance from an integrated PET/MRI system for small animals. Ann Nucl Med. 2010 Jan 8. [Epub ahead of print] [ ]. 3. von Schulthess GK, Schlemmer HP. A look ahead: PET/MR versus PET/CT. Eur J Nucl Med Mol Imaging. 2009;36 Suppl 1:S3-9. [ ] 4. West J, Fitzpatrick JM, Wang MY, et al. Comparison and evaluation of retrospective intermodality brain image registration techniques. J Comput Assist Tomogr. 1997;21:554-66. [ ] 5. Petersen RC, Doody R, Kurz A, et al. Current concepts in mild cognitive impairment. Arch Neurol. 2001;58:1985-92. [ ] 6. Silverman DH, Small GW, Chang CY, et al. Positron emission tomography in evaluation of dementia: regional brain metabolism and long term outcome. JAMA. 2001;286:2120-7. [ ] 7. Jellinger KA. The pathology of ischemic-vascular dementia: an update. J Neurol Sci. 2002;203-204:153-7. [ ] 8. Goffin K, Dedeurwaerdere S, Van Laere K, et al. Neuronuclear assessment of patients with epilepsy. Semin Nucl Med. 2008;(38):227-39. [ ] 9. Salamon N, Kung J, Shaw SJ, et al. FDG-PET/MRI coregistration improves detection of cortical dysplasia in patients with epilepsy. Neurology. 2008;71:1594-601. [ ] 10. Eidelberg D, Moeller JR, Ishikawa T, et al. Early differential diagnosis of Parkinson's disease with 18F-fluorodeoxyglucose and positron emission tomography. Neurology. 1995;45:1995-2004. [ ]
Received February 1, 2010.
* Study developed at Clínicas de Diagnóstico Por Imagem (CDPI) and Multi-Imagem PET, Rio de Janeiro, RJ, Brazil. |
|

{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554