Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 3 - May / June of 2010
Vol. 43 nº 3 - May / June of 2010
|
ORIGINAL ARTICLE
|
|
Uterine arteries resistance and pulsatility indices at the first and second trimesters of normal pregnancies |
|
|
Autho(rs): Antonio Gadelha da Costa, Patricia Spara, Thiago de Oliveira Costa, William Ramos Tejo Neto |
|
|
Keywords: Doppler effect, Uterine artery, Preeclampsia |
|
|
Abstract:
IPost-Doctorate, Professor at Universidade Federal de Campina Grande (UFCG), Campina Grande, PB, Brazil
INTRODUCTION Preeclampsia and intrauterine growth restriction (IUGR) are clinical entities that increase perinatal morbidity and mortality. Preeclampsia is related to a failure in the trophoblast invasion in the endometrial and myometrial vascularization, affecting the second wave of trophoblastic migration(1). Consequently, modifications occur in the uteroplacental blood flow, with a higher risk for developing preeclampsia, IUGR and small-for-gestational-age fetuses(2). Such abnormalities can be evaluated by Doppler velocimetry, considering that the histological modifications are compatible with changes in dopplervelocimetric parameters in preeclamptic patients(3). It is already well established that persistence of bilateral uterine artery notch after 26 weeks of gestation is predictive of pre-eclampsia. Uterine arteries diastolic notch at the second and third trimesters of gestation is related to increased uteroplacental vascular resistance. In such cases, a greater incidence of proteinuria, hypertension, IUGR and fetal hypoxia is observed(4). Currently, Doppler velocimetry of uterine arteries at the first and second trimesters of gestation and its relation with preeclampsia prediction has been under study. In 2008, Plasencia et al.(5) reported the relation between changes in pulsatility index (PI) at 11 to 13 weeks + 6 days to 21 to 24 weeks + 6 days and the occurrence of preeclampsia, particularly before 34 weeks. In this same research line, Melchiorre et al.(6) had observed association between resistance index (RI) and the presence of early preeclampsia, so considered when the delivery occurred before 37 weeks of gestation. Such authors have observed, greater RI in patients who developed preeclampsia in the first trimester of gestation than in healthy patients. In spite of various studies developed over the past 25 years, there is no consensus in literature on the values of doppler-velocimetric parameters for uterine arteries at the first, second and third gestational trimesters. Following the current trend towards dopplervelocimetric evaluation of uterine arteries at the first and second trimesters of gestation and, considering the relevance of this theme, it is important to determine the RI and PI in these maternal vessels in the two first trimesters of gestation. Therefore, the objective of the present study is to determine the values of RI and PI in uterine arteries of pregnant women considered as clinically healthy at the first and second gestational trimesters, correlating them with the presence or absence of notches.
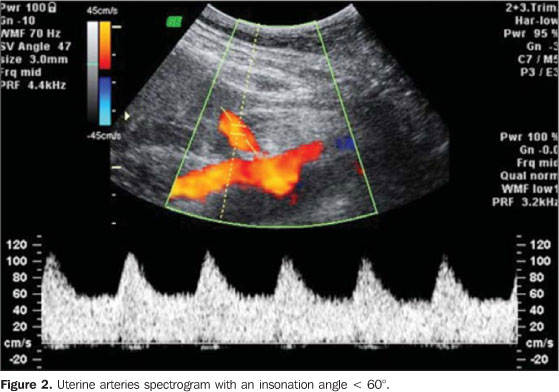
MATERIALS AND METHODS A prospective longitudinal study with 44 healthy pregnant women with ages between 18 and 35 years was developed from July 2007 to March 2009. The first Doppler ultrasonography study was performed in the 44 patients between the 8th and 12th gestational weeks, during which the gestational age was calculated based on the crown-rump length (CRL), and RI and PI of maternal arteries were measured. The subsequent studies were performed in 29 patients, at the 22nd gestational week, when the PI was measured again. The present study was approved by the Committee for Ethics in Research of Universidade Estadual da Paraíba, PB, Brazil, and all the patients signed a term of free and informed consent. The gestational age was established by the date of last menstruation and/or by the CRL measured by ultrasonography between the 8th and 12th gestational weeks, thus obtaining greater reliability in the gestational age calculation. In case of discrepancies between the gestational age calculated by the date of last menstruation and by CRL, the latter prevailed. Inclusion criteria were the following: single gestation; initial gestational age from the 8th to the 12th week; clinical and laboratory tests within normality parameters; and patients' agreement in participating in the study, after signature of the term of free and informed consent. Exclusion criteria were the following: presence of fetal malformation; smokers, alcohol or illicit drug users; partial or total follow-up discontinuation, since the study is of the longitudinal type. Evaluations regarding labor and the newborn had the objective of consolidating data on perinatal normality. The examinations were performed by a single observer, utilizing a Voluson 730 Pro ultrasonography apparatus (General Electric; Austria) with a convex multifrequency transducer (3.0 to 5.0 MHz). The patient was positioned in dorsal decubitus, semi-sitting position, at an angle between 15° and 30°, so as to avoid vena cava compression. Subsequently, a gel was applied on the transducer and the images and Doppler mapping were acquired. After image acquisition the dopplervelocimetric measurements of the maternal uterine arteries were performed, immediately after the iliac vessels crossing (Figure 1). Insonation angles < 60° were utilized, as well as wall filters at 50-70Hz frequencies and 1-2 mm sample volume, positioned at the center of the vessel, where the flow velocities are linear and coherent (Figure 2). Doppler-velocimetric parameters were obtained following spectral analysis of the uterine arteries, after obtention of five stable waves (Figure 2). Three RI and PI measurements were obtained at each examination, with the final result corresponding to the arithmetic mean of the three measurements for each dopplervelocimetric variable. Such parameters were obtained in 44 patients between their 8th and 12th gestational weeks and in 29 patients at the 22nd gestational week.
The software GraphPad StatMate 1.01i was utilized in the sample calculation, with the results from 19 patients in the preliminary phase of data collection, based on the difference of the mean value between the highest and lowest value of each dependent variable, using the highest standard deviation. For a 95% test power, 5 cases would be required for RI and 10 cases for PI. A higher number of patients were evaluated, considering the longitudinal nature of the study with the predictable possibility of patients loss along the study development. The statistical analysis was performed by measures of central distribution and dispersion and by the Student's t test, considering p < 0.05 as significance level. Measures of central distribution and dispersion were performed in order to determine the mean values and the standard deviation for each analyzed variable while the Student's t test was performed to compare two dependent variables. Dependent variables we uterine arteries RI and PI, and the independent variable was the gestational age from the 8th to 12th weeks and at the 22nd week.
RESULTS Forty four pregnant women with ages ranging from 18 to 35 years were evaluated. The deliveries occurred between the 38th and 41st weeks of gestation. The newborns´ weight ranged from 2,800 to 3,930 g and the height ranged from 46 to 53 cm. The Apgar score at the first minute ranged from 7 to 10, and at the fifth minute, from 9 to 10 (Table 1).
Uterine arteries RI and PI at the first trimester of gestation were higher than at the second trimester (p < 0.05 - Student's t). At the first trimester, the RI and the PI of uterine arteries with notches were 0.83 ± 0.07 and 2.32 ± 0.79 respectively, and without notches, 0.71 ± 0.16 and 1.61 ± 0.78. At the second trimester, RI and PI of the uterine arteries with notches were 0.59 ± 0.09 and 1.03 ± 0.32 respectively, and without notches, 0.44 ± 0.09 and 0.63 ± 0.19. At the first trimester, 37 (84.1%) of the patients presented bilateral notches, 2 (4.6%) presented unilateral notches and 5 (11.3%) did not present notches. At the 22nd gestational week, 5 (17.2%) presented bilateral notches, 8 (27.6%) presented unilateral notches and 16 (55.2%) did not present notches. Of the 29 patients that were followed-up until the conclusion of the present study, 27 presented notches at the first trimester. In 15 (55.5%) cases, the notches disappeared in the second trimester of gestation. No differences were observed as the dopplervelocimetric values of the left uterine artery when compared with those of the right uterine artery (p > 0.05 - Student's t). The intraobserver variability of the dopplervelocimetric measurements, according to the variation coefficient, was 4.51 for RI and 8.25 for PI (CI: 95%).
DISCUSSION Campbell et al.(4) were pioneers in the presentation of data on uteroplacental circulation by means of the study of arcuate arteries with Doppler velocimetry, having reported that the diastolic notch of uterine arteries at the second and third trimesters of gestation, was related to the increase in uteroplacental vascular resistance, IUGR and hypertension. Current studies report association between RI and PI values at the first gestational trimester, and the subsequent development of preeclampsia, particularly in cases where it occurs before the 37th gestational week(6,7). Plasencia et al.(5) have observed that, in normal pregnancies, there is a significant decrease of PI from 11th to 13th weeks + 6 days of gestation, as well as from 21st to 24th weeks + 6 days of gestational age. In the present study decreases in RI and PI were observed from 8 to 12 to 22 weeks of gestation. Such decrease occurred both in the presence and in the absence of uterine artery notches. Dopplervelocimetric parameters values for uterine arteries were lower in the absence of notches. Liao et al.(8) have determined PI values by means of transvaginal ultrasonography in healthy pregnant patients, during the period between 11 and 13 weeks + 6 days of gestation, as well as during the second gestational trimester, and observed that at the first trimester, 43.8% of the patients presented bilateral notch, 19.1% presented unilateral notch and 36.9% did not present notch. In the present study, most of the patients (84.1%) at the first gestational trimester presented bilateral notch, 4.6% presented unilateral notch and in 11.3% no notch was observed. As the present study is compared with that of Liao et al.(8), a difference is observed between the rates of bilateral notches in the uterine arteries during the first gestational trimester. Considering that the second wave of trophoblastic migration occurs between the 14th and 20th weeks of gestation(9,10), a period where uterine arteries notches disappear, it is understood that, at the first trimester, there must be a high rate of patients with bilateral notches in these arteries. Additionally, the present study is reproducible, considering that the intraobserver variability was below 10%, a value considered as appropriate for dopplervelocimetric measurements(11,12). In the present study, PI values for uterine arteries (1.61) at the first trimester of gestation are in agreement with those reported by Liao et al. (1.69)(8). Melchiorre et al.(6) have studied uterine arteries RI at the first trimester of gestation and reported the relation between the values of this dopplervelocimetric parameter and the development of preeclampsia before and after 37 weeks, which they denominated, respectively, early and late preeclampsia. Such authors have observed higher RI values in patients that developed early preeclampsia than in healthy patients. However, no difference was observed between the RI in healthy patients and those who developed preeclampsia after the 37th gestational week. The RI value for healthy patients was 0.70 ± 0.10, and in the patients who developed preeclampsia before the 37th week, 0.79 ± 0.12. In the present study, RI values for 8 to 12 weeks of gestation were 0.83 ± 0.07 for patients presenting bilateral notch, and 0.71 ± 0.16 in those that did not present notch. As the inclusion criterion for the study was healthy pregnant women, none of them developed preeclampsia. Therefore, increased RI of uterine arteries at the first trimester of gestation does not indicate development of preeclampsia. Additionally, in the results of the present study, it is evident that there is a decrease of RI when the uterine artery notches disappear. In the study developed by Melchiorre et al.(6) no relation was observed between RI values and the presence or absence of notch in the uterine arteries. Such authors report that the prevalence of bilateral uterine artery notches at the first trimester in patients with preeclampsia before 37 weeks (75.8%) was significantly higher than in healthy patients or in those with preeclampsia after 37 weeks of gestation. In the present study we observed that, at the first trimester of gestation, the majority of the patients (84.1%) presented bilateral notch. In 4.6% unilateral notch was found and in 11.3% notch was not observed. Therefore, the presence of bilateral uterine artery notch during the first trimester of gestation does not mandatorily indicate that there will be preeclampsia development. By analyzing the studies developed by Plasencia et al.(5) and Melchiorre et al.(6) , the authors of the present study observed that preeclampsia prediction by means of evaluation of RI and PI at the first trimester must be made by comparing doppler-velocimetric values of normal pregnant women with those from patients presenting a high risk for preeclampsia and/or small-for-gestational-age fetuses. Thus, it is important to determine the reference values for RI and PI of the uterine arteries in healthy pregnant women at the first trimester of gestation, in order to allow the comparison with those of high-risk pregnant women. In the present study, 17.2% of the patients at the 22nd week of gestation presented bilateral notch, 27.6% presented unilateral notch and 55.2% did not present any notch. It is observed that, at the second trimester of gestation, most of the normal pregnant women no longer present bilateral uterine artery notch. Liao et al.(8), studying healthy pregnant women from the 20th to the 24th week + 6 days of gestation, have reported that, during the second trimester of gestation, 4.3% presented bilateral notch, 9% presented unilateral notch, and 86.6% did not present any notch. In 2007, Toal et al.(13), evaluating high-risk pregnant women between the 19th and 23rd gestational weeks by means of Doppler of the uterine arteries, considered as abnormal results the presence of bilateral notch in these arteries and PI above 1.45. Papageorghiou et al.(14) have studied the Doppler velocimetry of maternal uterine arteries between the 22nd and 24th weeks of gestation, both from the qualitative point of view, by the presence or absence of bilateral notch, as well as quantitatively by the measurement of PI. The mean PI in patients that developed preeclampsia was 1.36 while that of patients that did not develop was 1.02. In 2009, along this same line of research, Liao et al.(8) evaluated the PI of healthy pregnant women during the period between the 22nd and 24th weeks and 6 days of gestation, observing that the mean PI was 1.03. In the present study, in which healthy pregnant women were evaluated at the 22nd week of gestation, the PI value of 1.03 was observed, in agreement with the values reported by Papageorghiou et al.(14) and Liao at al.(8). Additionally, the PI values were differentiated in the presence and absence of notch in maternal uterine arteries with the values of 1.03 ± 0.32 and 0.63 ± 0.19, respectively. If between the 20th and 24th weeks of gestation bilateral uterine artery notch is not observed, the patients are considered as being at low risk for preeclampsia and IURG. On the contrary, the presence of bilateral uterine artery notch at this gestational age is related to greater risk for development of preeclampsia and IURG(15). The present study involved low-risk pregnant women, and it was possible to observe that in healthy patients, uterine artery notches disappeared in 55.5% of the patients at the 22nd gestational week. However, in 44.5% uterine artery notch was present at the 22nd week of gestation, and no cases of preeclampsia development and/or IURG were observed. The importance of determining RI and PI of the uterine arteries in healthy pregnant women should be emphasized, so that these indices can be compared with those observed in high-risk patients. Additionally, the qualitative analysis by the presence or absence of uterine artery notch was correlated with the quantitative analysis by the determination of RI and PI of healthy pregnant women at the first and second trimesters of gestation.
CONCLUSION The RI and PI of uterine arteries are higher during the first trimester of gestation than at the second trimester. In approximately one half of the pregnant women uterine artery notch had disappeared at the 22nd week of gestation. The absence of uterine artery notch was related to decrease in RI and PI.
REFERENCES 1. Ganapathy R, Ayling LJ, Whitley GSJ, et al. Effect of first-trimester serum from pregnant women with high-resistance uterine artery Doppler resistance on extravillous trophoblast invasion. Hum Reprod. 2006;21:1295-8. [ ] 2. El-Hamedi A, Shillito J, Simpson NAB, et al. A prospective analysis of the role of uterine artery Doppler waveform notching in the assessment of at-risk pregnancies. Hypertens Pregnancy. 2005; 24:137-45. [ ] 3. Guzin K, Tomruk S, Tuncay YA et al. The relation of increased uterine artery blood flow resistance and impaired trophoblast invasion in pre-eclamptic pregnancies. Arch Gynecol Obstet. 2005;272:283-8. [ ] 4. Campbell S, Diaz-Recasens J, Griffin DR, et al. New doppler technique for assessing uteroplacental blood flow. Lancet. 1983;1:675-7. [ ] 5. Plasencia W, Maiz N, Poon L, et al. Uterine artery Doppler at 11 + 0 to 13 + 6 weeks and 21 + 0 to 24 + 6 weeks in the prediction of pre-eclampsia. Ultrasound Obstet Gynecol. 2008;32:138-46. [ ] 6. Melchiorre K, Wormald B, Leslie K, et al. First-trimester uterine artery Doppler indices in term and preterm pre-eclampsia. Ultrasound Obstet Gynecol. 2008;32:133-7. [ ] 7. Poon LC, Karagiannis G, Leal A, et al. Hypertensive disorders in pregnancy: screening by uterine artery Doppler imaging and blood pressure at 11-13 weeks. Ultrasound Obstet Gynecol. 2009;34: 497-502. [ ] 8. Liao AW, Toyama J, Costa V, et al. Correlation between the Doppler velocimetry findings of the uterine arteries during the first and second trimesters of pregnancy. Rev Assoc Med Bras. 2009;55: 197-200. [ ] 9. Brosens I, Robertson WB, Dixon HG. The physiological response of the vessels of the placental bed to normal pregnancy. J Pathol Bacteriol. 1967;93:569-79. [ ] 10. Sheppard BL, Bonnar J. The ultrastructure of the arterial supply of the human placenta in pregnancy complicated by fetal growth retardation. Br J Obstet Gynaecol. 1976;83:948-59. [ ] 11. Alcázar JL. Intraobserver variability of pulsatility index measurements in three fetal vessels in the first trimester. J Clin Ultrasound. 1997;25:366-71. [ ] 12. Hollis B, Mavrides E, Campbell S, et al. Reproducibility and repeatability of transabdominal uterine artery Doppler velocimetry between 10 and 14 weeks of gestation. Ultrasound Obstet Gynecol. 2001;18:593-7. [ ] 13. Toal M, Chan C, Fallah S, et al. Usefulness of a placental profile in high-risk pregnancies. Am J Obstet Gynecol. 2007;196:363.e1-7. [ ] 14. Papageorghiou AT, Yu CK, Erasmus IE, et al. Assessment of risk for the development of pre-eclampsia by maternal characteristics and uterine artery Doppler. BJOG. 2005;112:703-9. [ ] 15. Park YW, Lim JC, Kim YH, et al. Uterine artery Doppler velocimetry during mid-second trimester to predict complications of pregnancy based on unilateral or bilateral abnormalities. Yonsei Med J. 2005;46:652-7. [ ] Received December 22, 2009. * Study developed at Unit of Fetal Medicine - Universidade Federal de Campina Grande (UFCG), Campina Grande, PB, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554