Sr. Editor,
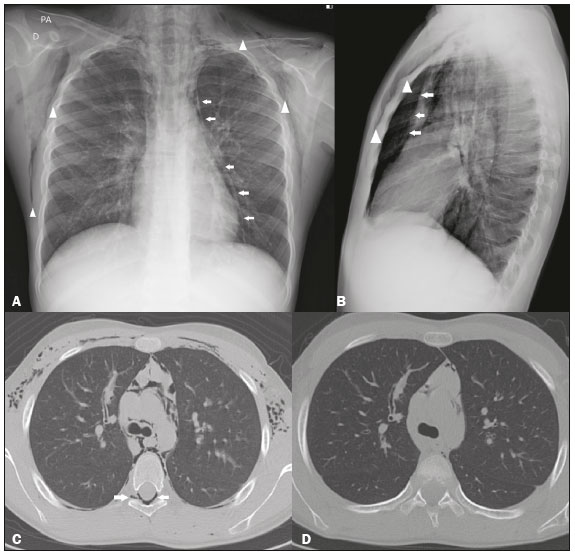
Paciente masculino, 11 anos, em tratamento irregular de asma, apresentando dispneia e dor torácica aguda, sem história de traumas recentes. No exame físico estava afebril, taquipneico, com crepitações na palpação do tórax, região cervical e axilar bilateral. Radiografia do tórax revelou pneumomediastino associado a enfisema subcutâneo bilateral nas partes moles do tórax e do pescoço (Figuras 1A e 1B), achados confirmados pela tomografia computadorizada (TC) de tórax, que também demonstrou presença de ar na região posterior do canal medular (pneumórraque) (Figura 1C). Depois de 72 horas houve melhora clínica do paciente, com redução do enfisema subcutâneo e importante reabsorção do pneumomediastino inicial (Figura 1D). Diante dos achados, foi feito o diagnóstico de síndrome de Hamman associada a pneumórraque.
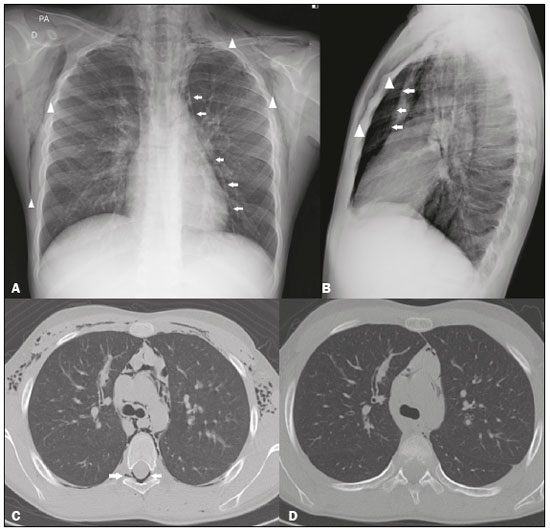 Figura 1.
Figura 1. Radiografias do tórax em posteroanterior (
A) e perfil (
B) mostrando pneumomediastino (setas) e enfisema de partes moles (cabeças de setas). A incidência em perfil identifica melhor o ar dissecando o mediastino anteriormente (setas). TC com janela intermediária com cortes ao nível da bifurcação brônquica na admissão do paciente (
C) e 72 horas depois (
D) demonstrando ar livre dissecando as estruturas mediastinais, brônquios e vasos pulmonares, além de pneumórraque (seta em
C). Observar a importante melhora do pneumomediastino, enfisema subcutâneo e pneumórraque 72 horas após a TC inicial (
D).
O pneumomediastino espontâneo ou síndrome de Hamman é definido pela presença de ar mediastinal livre na ausência de causa aparente, descartando-se traumatismos, iatrogenias e infecções por germes produtores de gás
(1). É uma afecção usualmente benigna, autolimitada, que afeta principalmente homens entre 17 e 25 anos, com incidência de 1/30.000 admissões hospitalares
(2).
A fisiopatologia dessa condição está baseada no efeito Macklin, caracterizado pela ruptura alveolar ocasionada por um gradiente de pressão entre os alvéolos e o interstício pulmonar, com consequente escape de ar para o interstício, que flui em direção ao hilo pulmonar e mediastino
(3,4). As principais causas de pneumomediastino espontâneo são exercício físico intenso, trabalho de parto, barotrauma pulmonar, mergulhos a grandes profundidades, tosse em paroxismos de forte intensidade, vômitos, asma, biotipo longilíneo, uso de drogas entorpecentes e após esforço vocal intenso
(2).
Os achados clínicos são dor torácica, dispneia, dor no pescoço e enfisema subcutâneo. Um sinal clínico característico que pode estar presente é o sinal de Hamman, que consiste na presença de crepitações sincronizadas com os batimentos cardíacos na ausculta. Este sinal é altamente sugestivo do quadro, mas está presente em menos da metade dos casos
(5). A associação com pneumórraque é infrequente e acredita-se que ocorra pela passagem de ar através dos planos mediastinais posteriores, atingindo os forames neurais e o espaço epidural
(6,7).
As radiografias do tórax ainda são o padrão ouro, com sensibilidade próxima a 100% quando realizadas as incidências posteroanterior e perfil
(2). Os principais achados incluem imagens lineares de gás no mediastino, geralmente seguindo até o pescoço, bolhas ou grandes coleções de ar delineando os vasos sanguíneos mediastinais, vias aéreas de grosso calibre, esôfago ou coração. A TC pode ser realizada na suspeita clínica quando a radiografia de tórax for normal ou inconclusiva, pois possibilita a localização anatômica do ar em cortes axiais e posteriores reconstruções. A TC também é o método de eleição para o diagnóstico e seguimento da pneumórraque
(8).
O tratamento é observação clínica associada a medidas de suporte, geralmente em meio hospitalar. Usualmente, ocorre a resolução espontânea do quadro entre dois e sete dias, e a recidiva é pouco frequente
(5).
Ainda que a síndrome de Hamman tenha baixa prevalência, deve ser considerada no diagnóstico diferencial de dor torácica aguda, principalmente em pacientes jovens com enfisema subcutâneo, podendo estar associada a pneumórraque.
REFERÊNCIAS1. Kelly S, Hughes S, Nixon S, et al. Spontaneous pneumomediastinum (Hamman''s syndrome). The Surgeon. 2010;8:63-6.
2. Lopes FPL, Marchiori E, Zanetti G, et al. Spontaneous pneumomediastinum following vocal effort: a case report. Radiol Bras. 2010;43:137-9.
3. Murayama S, Gibo S. Spontaneous pneumomediastinum and Macklin effect: overview and appearance on computed tomography. World J Radiol. 2014;6:850-4.
4. Conti-de-Freitas LC, Mano JB, Ricz HMA, et al. A importância da suspeita clínica da síndrome de Hamman na sala de urgência. Rev Bras Cir Cabeça Pescoço. 2009;38:122-3.
5. Fatureto MC, Santos JPV, Goulart PEN, et al. Pneumomediastino espontâneo: asma. Rev Port Pneumol. 2008;14:437-41.
6. Alves GRT, Silva RVA, Corrêa JRM, et al. Pneumomediastino espontâneo (síndrome de Hamman). J Bras Pneumol. 2012;38:404-7.
7. Borem LMA, Stamoulis DNJ, Ramos AFM. A rare case of pneumorrhachis accompanying spontaneous pneumomediastinum. Radiol Bras. 2017;50:345-6.
8. Oertel MF, Korinth MC, Reinges MH, et al. Pathogenesis, diagnosis and management of pneumorrhachis. Eur Spine J. 2006;15 Suppl 5: 636-43.
1. Hospital Santa Teresa, Petrópolis, RJ, Brasil
2. Instituto Estadual do Cérebro Paulo Niemeyer - Departamento de Radiologia, Rio de Janeiro, RJ, Brasil; a.
https://orcid.org/0000-0003-1483-27593. Instituto Estadual do Cérebro Paulo Niemeyer - Departamento de Radiologia, Rio de Janeiro, RJ, Brasil; b.
https://orcid.org/0000-0002-1936-3026Correspondência:Dr. Bernardo Carvalho Muniz
Instituto Estadual do Cérebro Paulo Niemeyer - Departamento de Radiologia
Rua do Resende, 156, Centro
Rio de Janeiro, RJ, Brasil, 20231-092
E-mail:
bernardocmuniz@yahoo.com.brRecebido para publicação em 21/08/2017
Aceito, após revisão, em 22/09/2017

 |
|



 Read in English
Read in English
 PDF Portuguese
PDF Portuguese
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket