Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 50 nº 1 - Jan. /Feb. of 2017
Vol. 50 nº 1 - Jan. /Feb. of 2017
|
LETTER TO THE EDITOR
|
|
Plasmacytoma of the trachea: a surprising diagnosis |
|
|
Autho(rs): Márcio Luís Duarte1; Mariana Carneiro Barbosa de Brito2; Fabricius André Lyrio Traple2; José Luiz Masson de Almeida Prado2; Luiz Carlos Donoso Scoppetta2 |
|
|
Dear Editor,
A 68-year-old man presented with a complaint of dyspnea on moderate exertion, and physical examination revealed stridor. The patient reported having previously been treated for chronic obstructive pulmonary disease and adenocarcinoma of the prostate, the latter having been treated with 39 radiotherapy sessions. He was a former smoker with a smoking history of 150 pack-years (3 packs/day for 50 years), having quit 4 years prior. We performed contrast-enhanced computed tomography (CT) of the neck and chest, which showed an expansive, well-defined nodular mass in the distal trachea, near the carina, without enhancement or signs of invasion of the tracheal walls (Figures 1 and 2). Bronchoscopy was requested for tumor resection, and symptom resolution was observed after the resection. The histopathological study identified an outer layer with the of appearance of plasmacytoid cells, sometimes with a central eosinophilic nucleolus"cartwheel appearance"and hyaline intracytoplasmic inclusions suggestive of Russell bodies. The immunohistochemical profile demonstrated positivity for CD3, CD20, CD45, CD56, kappa light chain, and CD138 in plasmacytes. In the context of the clinical status and test results, the findings were consistent with solitary extramedullary plasmacytoma. 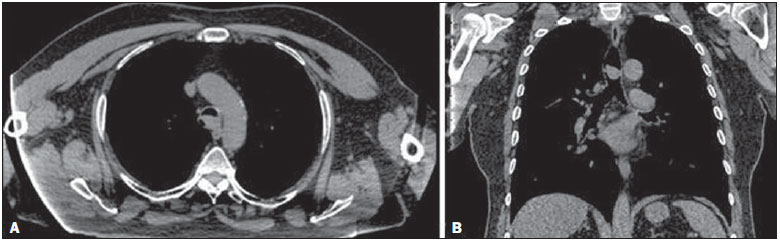 Figure 1. A: Axial CT scan, without contrast, showing an extensive, well-defined nodular mass in the distal trachea, measuring 2.1 × 1.3 × 1.7 cm, without signs of tracheal wall invasion. B: Coronal CT scan, without contrast, showing an expansive, well-defined nodular mass in the distal trachea, at the level of the carina, without signs of tracheal wall invasion. 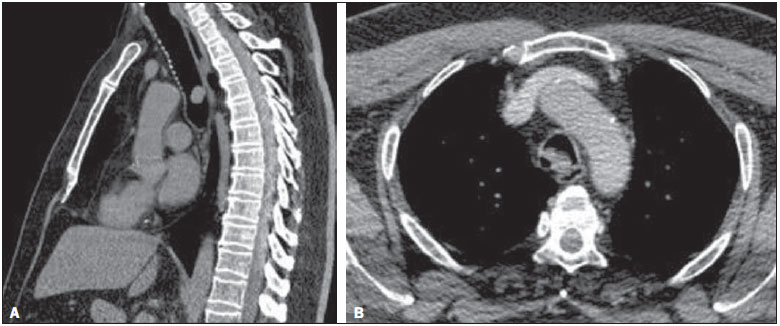 Figure 2. A: Sagittal CT scan (ROI: 51 HU), without contrast, showing an expansive, well-defined nodular mass in the distal trachea, without signs of tracheal wall invasion. B: Contrast-enhanced axial CT scan (ROI: 61 HU) showing an expansive nodular mass with no contrast uptake. Diseases involving the trachea or the main bronchi are not common(14). Less common still are tracheal tumors, which account for only 12% of all respiratory tract tumors(5,6), affecting mainly the lower third of the tract(7). Such tumors can be locally invasive(3), adenoid cystic carcinoma and squamous cell carcinoma being the malignant tumors most often affecting the trachea(5,6,8). The most common symptoms are related to airway obstruction, dyspnea being the most common, and become more evident when the tracheal lumen is narrowed by more than 75%(5,9). Other symptoms include cough, dysphonia, hoarseness, hemoptysis, stridor, dysphagia, nasal obstruction, epistaxis, rhinorrhea, ear pain, weight loss, and cyanosis(6). Extramedullary plasmacytoma of the trachea is a rare plasma cell malignancy (accounting for only 4% of plasma cell tumors), having been described in soft tissues outside the bone marrow, involving the submucosal lymphoid tissue, and occurring at different locations, especially in the upper airways, most often in the paranasal sinuses or nose(5,8,10). Involvement of the larynx, hypopharynx, cervical glands, esophagus, cervical lymph nodes, middle ear, and mastoid is rare(5), and tracheal involvement is even rarer(5,1113), occurring in only 3% of all extramedullary plasmacytomas(9). As of 2005, only 15 cases of solitary extramedullary plasmacytoma of the trachea had been reported in the medical literature(8). It primarily affects men between 50 and 60 years of age, with a male/female ratio ranging from 3:1 to 5:1(5,8). Progression to multiple myeloma is considerably less frequent than is solitary plasmacytoma of the bone(8). In ultrasound of the neck, tracheal lesions, especially those located anteriorly, can be visualized clearly(10). A CT scan allows the lumen, airway wall, and mediastinal structures to be evaluated. Multiplanar reconstructions are useful for assessing the type, degree, and longitudinal extent of the airway narrowing as well as the location of the tumor and its distance from the cricoid cartilage and carina(5,7). Bronchoscopy correlates well with CT and can be used in order to resect the lesion(5,7). The diagnosis is made through histological and immunohistochemical studies(5,14). There was one reported case in which the tracheal plasmacytoma was identified as an incidental finding on positron emission tomography/CT(5). The treatment can be surgical resection alone, radiotherapy alone, requiring annual monitoring, or a combination of the two(5,13,14). There is local recurrence in approximately 30% of cases and metastasis in 1540%(13). REFERENCES 1. Barbosa AGJ, Penha D, Zanetti G, et al. Foreign body in the bronchus of a child: the importance of making the correct diagnosis. Radiol Bras. 2016;49:3402. 2. Ribeiro GMR, Natal MRC, Silva EF, et al. Tracheobronchopathia osteochondroplastica: computed tomography, bronchoscopy and histopathological findings. Radiol Bras. 2016;49:567. 3. Barbosa BC, Amorim VB, Ribeiro LFM, et al. Tuberculosis: tracheal involvement. Radiol Bras. 2016;49:4101. 4. Franco RM, Guimaraes MD, Moreira BL, et al. Enhancing survival with early surgical resection of endobronchial metastasis in a follow-up of ovarian carcinoma. Radiol Bras. 2015;48:130. 5. Garelli M, Righini C, Faure C, et al. Imaging of a case of extramedullary solitary plasmacytoma of the trachea. Case Rep Radiol. 2011;2011: 687203. 6. Ferretti GR, Bithigoffer C, Righini CA, et al. Imaging of tumors of the trachea and central bronchi. Radiol Clin North Am. 2009;47:22741. 7. Olmedo G, Rosenberg M, Fonseca R. Primary tumors of the trachea. Clinicopathologic features and surgical results. Chest. 1982;81:7016. 8. Reyhan M, Tercan F, Ergin M, et al. Sonographic diagnosis of a tracheal extramedullary plasmacytoma. J Ultrasound Med. 2005;24:10314. 9. Dines DE, Lillie JC, Henderson LL, et al. Solitary plasmacytoma of the trachea. Am Rev Respir Dis. 1965;92:94951. 10. Sukumaran R, Nair RA, Jacob PM, et al. Extramedullary plasmacytoma of the trachea. Head Neck Pathol. 2014;8:2204. 11. Rai SP, Kumar R, Bharadwaj R, et al. Solitary tracheal plasmacytoma. Indian J Chest Dis Allied Sci. 2003;45:26972. 12. Kober SJ. Solitary plasmacytoma of the carina. Thorax. 1979;34:5678. 13. Kairalla RA, Carvalho CRR, Parada AA, et al. Solitary plasmacytoma of the trachea treated by loop resection and laser therapy. Thorax. 1988; 43:10112. 14. Dulmet E, Verley JM, Levasseur P, et al. Solitary plasmacytoma of the trachea. Apropos of a case. Ann Pathol. 1990;10:2757. 1. WebImagem, São Paulo, SP, Brazil 2. Hospital São Camilo, São Paulo, SP, Brazil Mailing address: Dr. Fabricius André Lyrio Traple Avenida Pompeia, 1178, Vila Pompeia São Paulo, SP, Brazil, 05022-001 E-mail: fabricius_traple@yahoo.com.br |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554