Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 5 - Sep. / Oct. of 2015
Vol. 48 nº 5 - Sep. / Oct. of 2015
|
LETTER TO THE EDITOR
|
|
Chordoid glioma of the third ventricle |
|
|
Autho(rs): Marília Henrique Destefani1; Alessandro Spanó Mello2; Ricardo Santos de Oliveira3; Gustavo Novelino Simão2 |
|
|
Dear Editor,
A previously healthy 27-year-old man was referred with an 8-month history of headaches, memory loss, progressive weight gain (obesity), hyperphagia and behavior changes. Computed tomography (CT) scans revealed the presence of a midline, solid, and homogeneously enhancing mass involving the anterior aspect of the third ventricle. Brain magnetic resonance imaging (MRI) (Figure 1) showed a well-defined, rounded mass in the third ventricle, measuring about 4.0 cm in the craniocaudal axis. The tumor was slightly heterogeneous, predominantly isointense at T1- and T2-weighted MRI sequences, presenting with diffuse enhancement after gadolinium injection. Perilesional vasogenic edema, compression and subsequent displacement of midbrain and hypothalamic structures were observed. 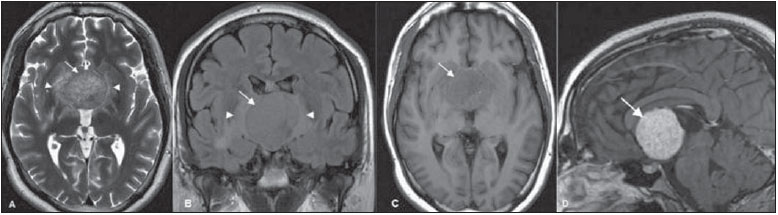 Figure 1. Axial MRI T2-weighted (A) and coronal FLAIR (B) sequences reveal a slightly hyperintense, well-defined hypothalamic/third ventricular tumor (arrows), with perilesional vasogenic edema (arrowheads). C: Axial MRI T1-weighted sequence reveals a predominantly isointense tumor (arrow). D: Gadolinium-enhanced sagittal MRI T1-weighted sequence reveals the tumor with uniform contrast enhancement (arrow). A subtotal resection of the tumor was microsurgically performed by interhemispheric transcallosal approach to the third ventricle. The tumor was histologically classified as a chordoid glioma. The mass showed nests of regular epithelioid cells with large nuclei, prominent nucleoli, and abundant eosinophilic cytoplasm, within a myxoid stroma. Sparse lymphocytic infiltrate was present. Immunohistochemical studies demonstrated diffuse cytoplasmic expression for glial fibrillary acidic protein, vimentin, and CD34. The patient died three months after surgery as a consequence of massive hypothalamic invasion combined with pneumonia. Chordoid glioma is an unusual, noninvasive and slow-growing tumor that arises from the anterior third ventricle, frequently adherent to the hypothalamus(1). There are reports in the literature about chordoid gliomas in other locations, such as the temporoparietal region, left thalamus and the corona radiata/thalamus(2,3), most of them affecting children(2). It is typically a well-circumscribed, round or oval-shaped tumor, with greatest diameter in the craniocaudal direction. The tumor is hyperdense to the gray matter at CT, isointense at MRI T1-weighted sequences, and isointense to slightly hyperintense at MRI long-TR, with strong, uniform enhancement after contrast agent administration(1,2,4-6). Cystic changes and necrosis may be present(2,5,7). Calcifications are usually rare(2,5,7). Usually, bilateral and symmetric perilesional vasogenic edema may also be observed(3-5). Given the tumor location, patients usually present with signs and symptoms related to obstructive hydrocephalus, such as nausea and headache, although endocrine imbalance, visual disturbances, behavior disorders and autonomic dysfunction are also reported in the literature(1,4-6). The histological and immunohistochemical features of these tumors are very typical and uniform, characterized by cords of oval to polygonal epithelioid cells with abundant eosinophilic cytoplasm and avid staining for glial fibrillary acidic protein and vimentin(1,2,4). The differential diagnosis includes masses of suprasellar region, such as pituitary macroadenoma, craniopharyngioma, optic and hypothalamic pilocytic astrocytoma, meningioma, ependymoma and lymphoma(2,4). Currently, the treatment of choice is complete surgical resection of the tumor(1,4,6). Adjuvant radiotherapy has been used following subtotal resection(2). Despite being a low-grade tumor, the prognosis is usually poor because of its location and the difficulty in obtaining complete surgical resection without causing severe hypothalamic symptoms(4). On the other hand, partial resection of the tumor is associated with high recurrence rates(4-6). REFERENCES 1. Ortega-Martínez M, Cabezudo JM, Bernal-García LM, et al. Glioma cordoide del III ventrículo. Nuevo caso y revisión de la literatura. Neurocirugía. 2007;18:115-22. 2. Desouza RM, Bodi I, Thomas N, et al. Chordoid glioma: ten years of a low-grade tumor with high morbidity. Skull Base. 2010;20:125-38. 3. Ni HC, Piao YS, Lu DH, et al. Chordoid glioma of the third ventricle: four cases including one case with papillary features. Neuropathology. 2013;33:134-9. 4. Pomper MG, Passe TJ, Burger PC, et al. Chordoid glioma: a neoplasm unique to the hypothalamus and anterior third ventricle. AJNR Am J Neuroradiol. 2001;22:464-9. 5. Smith AB, Smirniotopoulos JG, Horkanyne-Szakaly I. From the radiologic pathology archives: intraventricular neoplasms: radiologic-pathologic correlation. Radiographics. 2013;33:21-43. 6. Zarghouni M, Vandergriff C, Layton KF, et al. Chordoid glioma of the third ventricle. Proc (Bayl Univ Med Cent). 2012;25:285-6. 7. Glastonbury CM, Osborn AG, Salzman KL. Masses and malformations of the third ventricle: normal anatomic relationships and differential diagnoses. Radiographics. 2011;31:1889-905. 1. Cedirp - Radiologia e Diagnóstico por Imagem, Ribeirão Preto, SP, Brazil 2. Hospital das Clínicas - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (HCFMRP-USP), and Cedirp - Radiologia e Diagnóstico por Imagem, Ribeirão Preto, SP, Brazil 3. Hospital das Clínicas - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (HCFMRP-USP), Ribeirão Preto, SP, Brazil Mailing Address: Dra. Marília Henrique Destefani Avenida Professor João Fiusa, 2055, Jardim Irajá Ribeirão Preto, SP, Brazil, 14024-260 E-mail: mariliadestefani@ymail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554