Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 2 - Mar. / Apr. of 2015
Vol. 48 nº 2 - Mar. / Apr. of 2015
|
LETTER TO THE EDITOR
|
|
Biliary colon: an unusual case of intestinal obstruction |
|
|
Autho(rs): Ernesto Lima Araujo Melo1; Francisco Thiago Martins de Paula1; Rainne André Siqueira1; Sariane Coelho Ribeiro2 |
|
|
Dear Editor,
A female, 80-year-old, diabetic, hypertensive and obese patient reported sudden onset of colicky pain in the hypogastrium for two days. Also, there was association with nausea, and the patient was unable to eliminate feces and pass gas, besides presenting with abdominal distension. Physical examination demonstrated increased abdominal volume, pain to deep palpation of the hypogastrium, abdominal tympanism to percussion and signs of mild dehydration. The clinical hypothesis of obstructive syndrome was raised. Abdominal radiographic and sonographic images acquired in other service were not conclusive as regards the cause of the condition. Anteroposterior radiography in orthostasis and horizontal dorsal decubitus position demonstrated the presence of obstruction with predominantly gaseous distension of small bowel loops and part of the large bowel, with no signs of pneumoperitoneum. Ultrasonography demonstrated gaseous distension with no signs of free fluid at the moment of the study. With such studies indicating low obstruction with no defined cause, one has opted for performing abdominal computed tomography (CT) in order to clarify the diagnosis and define the therapeutic approach. Due to the clinical suspicion of neoplastic obstruction, the patient was referred to the authors' institution. With the CT study, the diagnosis could be established, and the several image reconstruction techniques - multiplanar, curve and 3D reconstruction - were utilized so as the findings could be presented to the requesting physician in a more easily understandable way. CT demonstrated the fistulous tract communicating the gallbladder lumen with the lumen of the transverse colon and the presence of a residual calculus in the gallbladder (Figure 1A). Curve reconstruction of the rectal and sigmoid colon region demonstrated an impacted calculus obstructing the sigmoid colon and causing abdominal distension upstream due to fecal buildup (Figure 1B). Endoluminal reconstruction of virtual colonoscopy images demonstrated the fistulous orifice in the transverse colon (Figure 2A). Tridimensional reconstruction for gaseous material demonstrated diffuse gaseous distension of the right, transverse and left colons, and also the site of the choledochal-colonic fistula (Figure 2B). Once the diagnosis was established, the patient was successfully submitted to surgery. 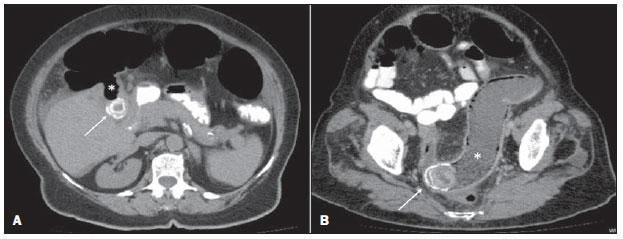 Figure 1. A: Axial CT image demonstrating the presence of a calculus in the gallbladder (arrow) and fistulous tract communicating the gallbladder with the large bowel (asterisk). B: Curve reconstruction of CT image demonstrating impacted biliary calculus in the sigmoid colon (arrow) and bowel distension upstream (asterisk). 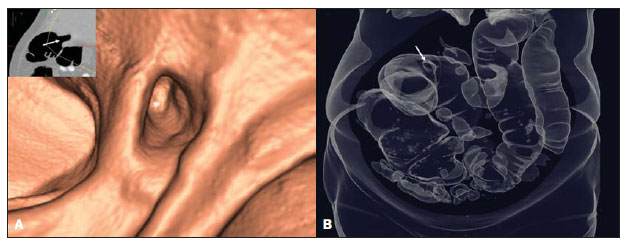 Figure 2. A: Endoluminal 3D reconstruction of virtual colonoscopy image demonstrating the fistulous orifice (asterisk) in the large bowel. The reference 2D image of the orifice positioning is highlighted (arrow). B: 3D reconstruction demonstrating gaseous bowel distention and the fistulous orifice (arrow). Acute obstructive cholecystitis may approach the serosas of the biliary and intestinal tracts due to the gallbladder and/or common biliary duct dilatation. With the repetition of inflammatory episodes and adherence of the serosas, choledochal-colonic fistularization may occur, allowing for the passage of biliary calculi into the intestinal lumen(1), besides calculi impaction at some point in the tract, causing significant pain, severe local irritation, edema or gangrene(2). Amongst cholecystointestinal fistulas, cholecystoduodenal fistulas represent more than 70%, while cholecystocolonic fistulas represent 8% to 26% of them(3). Rigler et al. established four criteria (presence of air or contrast medium in the biliary tract; direct or indirect identification of calculus in the bowel; alteration in the position of a previously identified calculus; radiological signs of either partial or total occlusion of the intestinal lumen) which corroborate a diagnosis of bowel obstruction caused by a calculus(4). Three findings determined by such criteria constitute the Rigler's triad: signs of small bowel dilation, pneumobilia and ectopic calculi. Despite the rarity of this condition, one should be attentive to the possibility of biliary colon in acute onset of lower intestinal obstruction, in order to allow for a prompt and correct diagnosis and institution of an appropriate treatment. REFERENCES 1. Wang JK, Foster SM, Wolff BG. Incidental gallstone. Perm J. 2009;13:50-4. 2. Costi R, Randone B, Violi V, et al. Cholecystocolonic fistula: facts and myths. A review of the 231 published cases. J Hepato Biliary Pancreat Surg. 2009;16:8-18. 3. Del Gaizo A, Raval B. Cholecystocolonic fistula. Applied Radiology. 2006;35:21-2. 4. Smyth J, Dasari BV, Hannon R. Biliary-colonic fistula. Clin Gastroenterol Hepatol. 2011;9:A26. 1. Universidade Estadual do Ceará (UECE), Fortaleza, CE, Brasil 2. Hospital Israelita Albert Einstein, São Paulo, SP, Brazil Mailing Address: Dr. Ernesto Lima Araujo Melo Universidade Estadual do Ceará, Centro de Ciências da Saúde - Curso de Medicina Avenida Paranjana, 1700, Campus do Itaperi Fortaleza, CE, Brasil, 60740-000 E-mail: ernesto.melo@uece.br |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554