Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 5 - Sep. / Oct. of 2014
Vol. 47 nº 5 - Sep. / Oct. of 2014
|
ORIGINAL ARTICLE
|
|
Determination of dosimetric quantities in pediatric abdominal computed tomography scans |
|
|
Autho(rs): Tiago da Silva Jornada1; Teógenes Augusto da Silva2 |
|
|
Keywords: Pediatric computed tomography scans; Dosimetric quantities; Weighted dose index; Volumetric air kerma index; Air kermalength product. |
|
|
Abstract: INTRODUCTION
Developments in computed tomography (CT) as a medical imaging method, and its constant technological advances over the years have expanded its application; currently, CT became one of the most relevant radiological techniques easily accessible to the greatest part of the population(1). The pediatric patient group has increased in this population over the years; for example, in 1980, 3 million CT scans were performed in the United States of America (USA) and in 1996 it reached 62 million with 4 million in children(1). It is estimated that 10% of all CT scans performed in the world involve pediatric patients(2). The consequence of the dissemination of this technique in the medical practice is an increase in the collective dose due to patient exposures, since the doses are much higher than those from the exposures related to any other conventional radiology technique(3). According to many epidemiological studies, the significant increase in the number of CT scans associated with the increase in dose should presumably lead to a higher probability of development of harmful effects, particularly in children(4-7). The current scenario raises the necessity of a radiological protection policy aiming at the knowledge and control of radiation doses involved in pediatric CT procedures. The first international discussion focused on the radiological protection of patients occurred in 2001 during the Conference of Malaga, approaching radiotherapy and radiodiagnosis procedures as well as those related to nuclear medicine(8). The most frequent method used to estimate doses in CT consists in measurements with either a ionization chamber positioned free-in-air or inserted into a head or neck phantom; the computed tomography dose index (CDTI) is determined and adopted as reference(9). The International Atomic Energy Agency (IAEA) suggests the use of the term "air kerma índex" (Ca) replacing CTDI, but the two dosimetric quantities are obtained by a same procedure and have a same numeric value(8). The purpose of knowing the dosimetric quantity values is to allow the comparison between such values and the diagnostic reference levels (DRL). DRLs are utilized as reference tools for quality control of the technique, but should not be used as exact values adopted with the purpose of dose restriction. The DRL objective is to avoid radiation dose to the patient that does not contribute to the clinical purpose of a medical imaging procedure, indicating the necessity of an optimization process(10). The concern with radiation levels in pediatric CT scans has stimulated actions aimed at radiological protection of children, among them the Image Gently campaign in the USA(11). The California state has sanctioned a regulation establishing the inclusion of dosimetric quantity values involved in tomographic procedures in the patients' medical records(12). In Brazil, no similar action has been adopted by the authorities. Furthermore, studies approaching dosimetric quantity values in tomographic procedures practically do not exist(13). The present study is aimed at quantifying dosimetric quantity values specific for CT, focusing on pediatric patients undergoing abdominal CT scans at two institutions in the city of Belo Horizonte, MG, Brazil. The objective is to study the application of dosimetric quantity values in the process of dose optimization, besides evaluating the conformity of such values with the diagnostic reference levels. MATERIALS AND METHODS The IAEA definitions(8) were adopted for the dosimetric quantities expressed in terms of kerma (kinetic energy released per unit mass). The weighted air kerma index (CW) (equation 1) has the objective of measuring the air kerma index within the phantoms; the volumetric air kerma index (CVOL) (equation 2) provides the estimate of the dose in a single section; the air kerma-length product (PKL,CT) (equation 3) provides the air kerma in the whole irradiated area during the acquisition of the tomographic image. The authors have also adopted the concept of effective dose estimated from PKL,CT as a function of a conversion factor k (equation 4; Table 1), depending only on the irradiated body region(14). 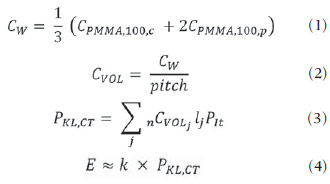 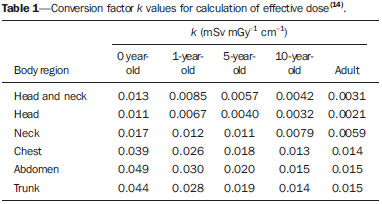 Air kerma rates were obtained within a cylindrical polymethyl metacrylate (PMMA) phantom with density 1.19 ± 0.01 g.cm-3, 16 cm in diameter and 15 cm in length, which is a pediatric trunk phantom indicated for patients in the age range from 1 to 15 years). The phantom was positioned and carefully aligned with the laser beam of the CT apparatus within the gantry. With the ionization chamber inserted between the peripheral and central holes of the phantom, three measurements were performed in terms of PKL, and the readings were duly corrected by the calibration factor NPKL,Q = 9.97 × 103 Gy.cm.unit-1(15), by the energy dependence factor (kQ = 1) and by the pressure and temperature factor (kTP = 0.9). The measurements of the dosimetric quantity were carried out in two devices of two hospitals where abdominal CT scans were performed in pediatric patients, as follows: a Toshiba Asteion single-slice and a GE BrightSpeed multi-slice machines. A 10X4-CT pencil-type Radcal® ionization chamber (100 mm in length and radius of approximately 3 mm) coupled with a 9060 model Radcal® electrometer was utilized to determine the air kerma rates in the center (CPMMA,100,C) and extremity holes of the phantom (CPMMA,100,p) in order to calculate the CW (equation 1). RESULTS With the single-slice CT equipment, the CW value was 18.73 ± 0.26 mGy, which, for the pitch of 1.2 adopted by the hospital, corresponds to the CVOL value of 14.61 mGy. The scan length for a pediatric abdominal CT is 22 cm over the patient's body, resulting in PKL,CT of 343.51 mGy.cm; this corresponds to an effective dose of 6.87 mSv, considering a conversion factor k = 0.020 (Table 1) for the abdominal region of a patient at the age of five years(15). With the multi-slice CT equipment, for a pitch of 0.9 and the same 22 cm scan length, the CW was 18.81 ± 0.22 mGy; the CVOL, 20.07 mGy; the PKL,CT, 441.64 mGy.cm; and the effective dose 8.83 mSv. DISCUSSION A comparison of the results obtained in the two CT devices showed that the difference between the CW values was not significant, but for CVOL, PKL,CT and effective dose, the increases of, respectively, 37%, 29% and 29% observed with the multi-slice equipment may be considered significant. Such a fact is explained by the pitch of 0.9 adopted by the hospital, which causes tomographic sections overlapping and, consequently, greater patient exposure to radiation. DRLs for pediatric abdominal CT scans in five-year-old patients are recommended as 25 mGy for CW, and 360 mGy.cm for PKL,CT (3). Both hospitals indicated values lower than the DRLs for such dosimetric quantities, except for the value of PKL,CT in the hospital with the multi-slice equipment, that remained 23% higher than the DRL, as shown on Figure 1. Considering that there is no tolerance range for DRL values, the result suggests that studies should be done in the hospital with the multi-slice equipment, in order to verify if an appropriate level of imaging quality could be achieved with lower levels of radiation doses. 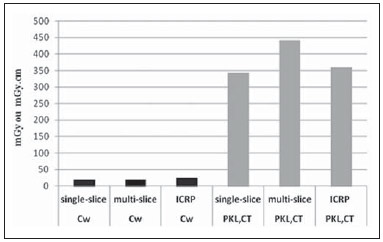 Figure 1. Comparison between values for CW and PKL,CT and DRL in pediatric abdominal CT scans. The increase of 2 mSv in the effective dose during the scan with the multi-slice equipment, as compared with the scan performed with the single-slice equipment, does not indicate the necessity of optimization, even considering that the first equipment offers better technological resources to provide patients with lower radiation doses without loss in the imaging quality. Until the present moment, none DRL was established in terms of effective dose for pediatric scans. The values obtained with surveys of the effective doses for abdominal scans in adult patients in some countries range from 5.3 to 13.2 mSv, with a median of 9.5 mSv(2). Such data suggest that the effective dose of 8.83 mSv observed in the multi-slice equipment is not appropriate for pediatric scans; the results suggest that there is room for improving the optimization in the hospital. CONCLUSIONS If only the dosimetric quantity CW is considered as a comparative tool, both hospitals would not need to implement an optimization process. However, as the PKL,CT values in the hospital with the multi-slice equipment are analyzed, one may conclude that an optimization of the technical procedures should be considered in order to reduce the radiation doses in pediatric abdominal CT scans. The effective dose value might be adopted as a criterion to be taken into account and for decision-making about the implementation of an optimization process; it should be considered that a tomographic image is to be obtained without loss in the diagnostic quality, but the radiation dose delivered to the patient should be as low as possible. CT scan dosimetry has at least four dosimetric quantities with specific objectives. The medical physicist responsible for determining their values should be aware of the differences among them and able to select the one that best fits his/her purpose. The consideration about the necessity of optimization based on a single dosimetric quantity may be limited. Acknowledgements To Comissão Nacional de Energia Nuclear (CNEN) for the Master scholarship granted to Tiago da Silva Jornada; to Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo à Pesquisa do Estado de Minas Gerais (Fapemig) for the financial support. The present study is part of the INCT Radiation Metrology in Medicine. REFERENCES 1. Brenner DJ, Hall EJ. Computed tomography - an increasing source of radiation exposure. N Engl J Med. 2007;357:2277-84. 2. Tack D, Gevenois PA. Radiation dose from adult and pediatric multidetector computed tomography. 1st ed. Berlin: Springer; 2007. 3. International Commission on Radiological Protection. Managing patient dose in computed tomography. ICRP Publication 87. Ann ICRP. 2000:30(4). 4. Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012;380:499-505. 5. Pierce DA, Preston DL. Radiation-related cancer risks at low doses among atomic bomb survivors. Radiat Res. 2000;154:178-86. 6. Brenner DJ. Estimating cancer risks from pediatric CT: going from the qualitative to the quantitative. Pediatr Radiol. 2002;32:228-41. 7. Brenner DJ, Elliston CD, Hall EJ, et al. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol. 2001;176:289-96. 8. International Atomic Energy Agency. Dosimetry in diagnostic radiology: an international code of practice. Technical Reports Series no. 457. Vienna: IAEA; 2007. 9. Maia AF. Padronização de feixes e metodologia dosimétrica em tomografia computadorizada. [Tese de doutorado]. São Paulo: Instituto de Pesquisas Energéticas e Nucleares; 2005. 10. Committee 3 of the International Commission on Radiation Units and Measurements. Diagnostic reference levels in medical imaging: review and additional advice. [acessado em 25 de outubro de 2012]. Disponível em: http://www.icrp.org/docs/DRL_for_web.pdf. 11. Image Gently - Education Materials. The alliance for radiation safety in pediatric imaging. [acessado em 12 de março de 2012]. Disponível em: http://www.pedrad.org/associations/5364/ig/Home.aspx. 12. UCDavis Health System. Radiation dose reporting. [acessado em 25 de janeiro de 2013]. Disponível em: http://www.ucdmc.ucdavis.edu/radiology/RadiationDose.html. 13. Vilarinho LM, Mota HC, Dias SK. Avaliação de doses em tomografia computadorizada pediátrica. [acessado em 25 de janeiro de 2013]. Disponível em: www.abfm.org.br/c2004/trabalhos/tupo236.pdf. 14. American Association of Physicists in Medicine. The measurement, reporting, and management of radiation dose in CT. AAPM Report No. 96. College Park, MD: AAPM; 2008. 15. IPEN. Laboratório de calibração de instrumentos LCI. Certificado de calibração nº 0577/2010. Data: 9 de junho de 2010 (impresso). 1. Master, PhD student in Clinical Radiology, Department of Imaging Diagnosis - Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 2. PhD, Senior Researcher, Comissão Nacional de Energia Nuclear (CNEN), Teacher of the Post-graduation Course at Centro de Desenvolvimento da Tecnologia Nuclear (CDTN/CNEN), Belo Horizonte, MG, Brazil Mailing Address: Dr. Teógenes Augusto da Silva Comissão Nacional de Energia Nuclear - Centro de Desenvolvimento da Tecnologia Nuclear Avenida Presidente Antonio Carlos, 6627, Campus da UFMG, Pampulha Belo Horizonte, MG, Brazil, 31270-901. Caixa Postal: 941 E-mail: silvata@cdtn.br Received May 9, 2013. Accepted after revision April 15, 2014. Study developed at Post-graduation Program, Centro de Desenvolvimento da Tecnologia Nuclear (CDTN/CNEN), Belo Horizonte, MG, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554