Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 4 - July / Aug. of 2014
Vol. 47 nº 4 - July / Aug. of 2014
|
ORIGINAL ARTICLE
|
|
Reference intervals of fetal cisterna magna volume by two-dimensional method using the multiplanar mode of three-dimensional ultrasonography |
|
|
Autho(rs): Luciano Marcondes Machado Nardozza1; Ana Paula Passos2; Edward Araujo Júnior1; Rafael Frederico Bruns3; Antonio Fernandes Moron4 |
|
|
Keywords: Fetus; Cisterna magna; Reference intervals; Two-dimensional ultrasonography; Three-dimensional ultrasonography. |
|
|
Abstract: INTRODUCTION
The subarachnoid cisterns are spaces larger than the subarachnoid space, formed between the pia mater and the arachnoid membrane, whose cerebrospinal fluid accumulation is greater than in other regions. Main cisterns are: cisternamagna, pontine cistern, interpeduncular cistern and chiasmatic cisterna. The cisterna magna is located in the posterior fossa and occupies the space between the inferior aspect of the cerebellum, the posterior aspect of the bulb and the roof of the fourth ventricle. It caudally continues with the spinal subarachnoid space and connects with the fourth ventricle by means of its medial aperture(1). The evaluation of the fetal cisterna magna is of great importance, because of the presence of anomalies such as the Dandy-Walker complex and mega-cisterna magna. Dandy-Walker complex is characterized by a combination of ventriculomegaly, enlarged cisterna magna, cerebellar vermis agenesis and superior displacement of the tentorium(2,3). Mega-cisterna magna is defined as a cisterna magna > 10 mm in diameter, with no change in the cerebellar vermis(4). A great difficulty in the evaluation of posterior fossa anomalies refers to the diagnosis of cerebellar vermis rotation, which is not possible in the axial plane. Three-dimensional ultrasonography (3DUS) in the multiplanar mode allows for the simultaneous visualization of three orthogonal planes (axial, sagittal and coronal) besides the manipulation of such planes in the "x, y and z" axes(5), which, on its turn, allows for the evaluation of the embryonic development of the cerebellar vermis(6). Previously to the introduction of 3DUS, the volumetric evaluation of fetal structures was performed by means of two-dimensional ultrasonography (2DUS), suggesting that fetal organs presented with a regular geometrical shape resembling an ellipsoid. In spite of being a method with proven accuracy both in vitro and in vivo studies(7,8), 3DUS is still an expensive technique available only in few reference centers in the world, particularly in developed countries. For small fetal structures with little irregularities, 2DUS could be utilized for being an appropriate and low-cost method, besides being accessible to a higher number of clinicians and investigators(9,10). The present study was aimed at determining reference intervals for the fetal cisterna magna volume by means of the two-dimensional method, by utilizing the multiplanar mode of 3DUS, besides evaluating the method reliability and intraobserver agreement. MATERIALS AND METHODS A prospective and cross-sectional study was undertaken with healthy pregnant women between the 17th and 29th weeks, in the period between August of 2010 and January of 2012. The present study was approved by the Committee for Ethics in Research of Universidade Federal de São Paulo and all the participants signed a term of free and informed consent. The patients were randomly selected, and all exams were performed at Clínica Fetalmed, Curitiba, PR, Brazil. All the patients underwent a single examination, and their postnatal results were not obtained. The scans were performed by a single investigator, with three-year experience in 3DUS, utilizing a Voluson 730 Expert (General Electric Medical System; Zipf, Austria) apparatus. The analyses were performed off-line with the aid of the software 4D views, release 10.0 (General Electric Medical System; Zipf, Austria). The inclusion criterion was the presence of single gestation with gestational age confirmed up to the 13th week by means of the crown-rump length. Exclusion criteria were following: presence of fetal malformations detected at ultrasonography; pregnant patients with chronic diseases (arterial hypertension, diabetes mellitus or collagen diseases); fetuses with weight prediction below the 10th. percentile or above the 90th percentile, according to the table proposed by Hadlock et al.(11); and presence of posterior acoustic attenuation caused by obesity or previous surgical scars. Initially, a real-time 2D scan was performed in order to obtain biometry, quantification of amniotic fluid and fetal morphological assessment. Subsequently, a 3D scan was carried out on the fetal central nervous system. With the purpose of optimizing the volumetric acquisition, an aperture angle between 50° and 70° was standardized, varying according to gestational age, normal velocity mode, high quality and harmonic mode. With the fetus at rest, and requesting the patient to hold the breath for a few seconds, the scanning window was opened in such a manner to comprise the entire fetal skull. The utilized standard plane for the volumetric acquisitions was the plane for measurement plane of the lateral ventricles. After volumetric acquisition, the image was presented in the multiplanar mode, in three orthogonal planes perpendicular to each other, as follows: axial (A acquisition plane), sagittal (B) and coronal (C). The A plane was selected as a reference and rotated in the craniocaudal direction by means of the Ref slice key, until the standard measurement plane of the transverse diameter of the cerebellum was obtained, as proposed by Goldstein et al.(12). For the volumetric measurement of the fetal cisterna magna by means of the 2D method, the axial and sagittal planes were utilized. Two linear measurements were made in the axial plane, one between the internal surface of the cerebellar vermis and the internal edge of the occipital bone (thickness) and superior and inferior poles of the cisterna magna, in relation to the transducer (width). A third measurement was performed in the sagittal plane, between the internal surface of the tentorium bone and the lower limit of the cisterna magna (length). The apparatus automatically calculated the volume of the structure, by multiplying such diameters by the constant value of 0.52 (Figure 1). Only one measurement of the fetal cranial volume was made per patient, and the values were recorded in the apparatus' memory and later transferred to compact discs.  Figure 1. Calculation of the fetal cisterna magna volume by the 2D method, utilizing the multiplanar mode of three-dimensional ultrasonography. Width (D1 = 2.69 cm) and length (D2 = 0.95 cm) will be marked in the axial plane; and height (D3 = 2.17 cm), in the sagittal plane. Automatically, the apparatus calculates the volume by means of the product of the three distances, multiplied by the constant 0.52 constant. The sample size calculation was based on the concept proposed by Royston by which for the construction of fetal reference intervals requiring 90% of variation between the 5th and 95th percentiles, a sample of 20 per week is recommended(13). The data were transferred to an Excel 2007 (Microsoft Corp.; Redmond, USA) worksheet and were analyzed by the softwares PASW release 18.0 (SPSS Inc.; Chicago, USA) and GraphPad release 5.0 (GraphPad Software; San Diego, USA). For the descriptive analysis, mean values, median, standard deviation, maximum and minimum values for the cisterna magna 2D volume were calculated for each gestational age. For the construction of reference intervals for 2D fetal cisterna magna as a function of gestational age, polynomial regressions were made, and adjustments were performed by means of the determination coefficient (R2). The 5th, 50th and 95th percentiles were determined for each gestational age, as proposed by Altman et al.(14). For the calculations of reliability and agreement, the same investigator performed a second random measurement of 50 volumes with an interval of at least 30 days from the first measurement (for intraobserver agreement), while a second investigator with similar experience in 3DUS, performed a third measurement of the same 50 volumes. Both investigators were blinded to each other's results. The intraclass correlation coefficient (ICC) was utilized for the evaluation of intra- and interobserver agreement, while the agreement limits and Bland-Altman plots(15) of the relative differences were utilized in the evaluation of intra- and interobserver agreement. A significance level of p < 0.05 was utilized in all the analyses. RESULTS Initially, the authors initially selected 233 cases, but 9 of those cases were excluded 2 cases of structural malformations detected at ultrasonography, 5 cases with weight prediction below the 5th percentile 5; 1 case with weight prediction above the 90th percentile, and 1 case because of technical difficulties. Therefore, 224 cases were considered for the final statistical analysis. Mean gestational age was 23.78 ± 3.60 weeks. Mean maternal age was 29.32 ± 5.40 years (1342 years). The mean number of deliveries was 1.60 ± 0.78 deliveries (1-4 deliveries). As regards fetal gender, 48.9% were male and 51.1% were female. The mean value of the 2D cisterna magna volume ranged from 0.71 ± 0.19 cm3 (0.481.08 cm3) to 4.18 ± 0.75 cm3 (3.225.38 cm3) between the 17th and 29th gestational weeks, respectively. Correlation between the 2D fetal cisterna magna volume and gestational age (GA) was observed, better represented by the following quadratic equation: 1,918 + 0.0284 × GA + 0.0065 × GA2; R2 = 0.67 (Figure 2). Table 1 presents the 5th, 50th and 95th percentiles for each evaluated gestational age. 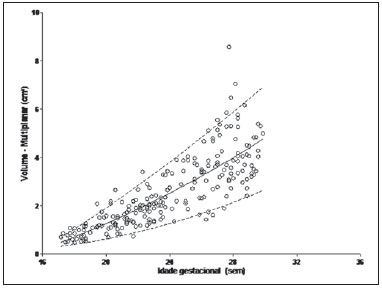 Figure 2. Scatter plot of correlation between volume of the fetal cisterna magna and gestational age, by means of the 2D method. 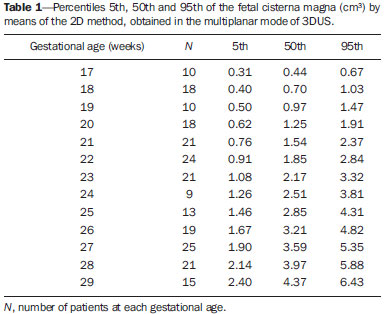 Good reliability and intraobserver agreement were observed, with ICC = 0.89 (CI 95%: 0.810.94) and mean relative difference 0.1% (agreement limits 95%: 52.0; 51.8), respectively (Figure 3). Low interobserver reliability and agreement were observed, with ICC = 0.64 (CI 95%: 0.450.78) and mean relative difference 16.9% (agreement limits 95%: 110; 84.6), respectively (Figure 4). 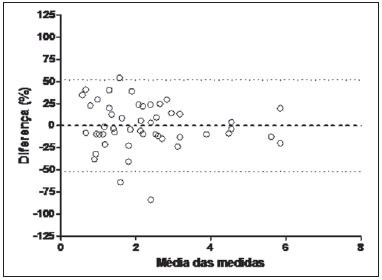 Figure 3. Bland-Altman graph showing the average of the relative difference between two measurements performed by a single investigator (intraobserver) plotted against the difference of his mean values for the 2D volume of the fetal cisterna magna. 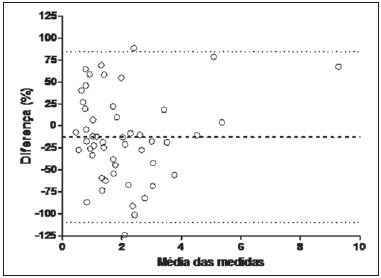 Figure 4. Bland-Altman graph showing the average of the relative difference of two measurements performed by two investigators (interobserver) plotted against the difference of their mean values for the 2D volume of the fetal cisterna magna. DISCUSSION In the present study, reference intervals were determined for the fetal cisterna magna volume by the 2D method, which, to the best of the authors' knowledge, have not been published in the literature. The authors utilized the interval from the 17th to the 29th weeks of gestation. The lower limit (the 17th week) was established due to the fact that the cerebellar vermis development is completed at the 18th week(16); thus, the measurement of its volume by the 2D method, particularly the measurements of the length, distance between the vermis and the occipital bone, could be compromised. The upper limit was established because of the difficulty to include the entire fetal skull in the scanning window at 3DUS (region of interest)(17). A total of 224 patients were evaluated, distributed in 14 gestational ages, providing an average of 16 patients, a very close value to that recommended by Royston(13) for the construction of reference intervals for fetal biometric parameters. There are only two articles in the literature determining reference intervals for the anteroposterior length of fetal cisterna magna, with no descriptions for its area or volume. In the study developed by Serhatlioglu et al.(18), 130 pregnant women between the 16th and 38th weeks of gestation were evaluated for the anteroposterior diameter of the fetal cisterna magna. Such authors have observed the increase of such a diameter with gestational age, represented by means of a quadratic equation of the same kind found in the present study for the 2D volume. The study developed by Serhatlioglu et al.(18) has demonstrated that the utilization of a fixed value of 10 mm to indicate anomalies of the posterior fossa may be subject to errors, depending on the evaluated gestational age. In the study developed by Koktener et al.(19), the authors have evaluated normal 194 fetuses between the 16th and 24th gestational weeks, and observed a linear correlation between anteroposterior diameter of fetal cisterna magna and gestational age; however, it is important to mention that those authors did not evaluate the third trimester of gestation, the period where there is a greater development of the cisterna magna. In the present study, the ellipsoid 2D volume was evaluated by utilizing the multiplanar mode of 3DUS. The multiplanar mode allows for the simultaneous visualization of the three orthogonal planes (axial, sagittal and coronal). In spite of not being essential for the volume measurement, the multiplanar mode presents the advantages of requiring less time, as with a single acquisition all necessary planes are obtained, and the possibility of performing the analysis in the absence of the patient. The volumes can also be sent to tertiary centers for analysis(20,21). Additionally, the utilization of the Ref slice key allows for the acquisition of the exact measurement plane(22), which is a difficulty observed at conventional 2DUS. As the cisterna magna, particularly in the second trimester, is a small and relatively regular structure, the ellipsoid 2D method could also be an alternative to 3DUS and magnetic resonance imaging (MRI). In the present study, good intraobserver reproducibility was observed; however, the interobserver reproducibility was low. The good intraobserver reliability and agreement were in part due to the learning curve, as the main investigator performed more than 200 volume measurements. The authors believe that the low interobserver reproducibility occurred mainly in the height measurement in the sagittal plane, distance from the interior surface of the tentorium bone to the lower edge of the cisterna magna. The visualization of such a limit is difficult, many times requiring adjustments in the measurement plane, a fact that may have contributed to the low reproducibility. Such a low interobserver reproducibility does not affect the quality of the reference curve determined in the present study. It only demonstrates the need for previous training of the investigator to perform appropriate measurements of its axes, and consequently, of its volume. As a positive point in the present study, the sampling size should be highlighted, as it is in accordance with the recommendations by Royston(13) for the construction of reference intervals for fetal biometrical parameters, besides reliability and agreement tests. The negative point is the absence of other method for comparison in the measurement of the fetal cisterna magna volume, particularly MRI. Such a method is the method of choice for evaluating the posterior fossa, as it does not suffer from interferences in terms of posterior acoustic shadowing from the bones in the skull base(23). Among the possible clinical applications of such a curve, one can mention those cases with borderline measurements (10 mm) of the fetal cisterna magna in the axial plane. In such cases, the volumetric evaluation by the 2D method can assist in the differentiation between normal and pathological cases, which would require specialized prenatal follow-up, in addition to parents counseling. In summary, the authors determined reference intervals for the fetal cisterna magna volume by means of the 2D method, utilizing the multiplanar mode of 3DUS. Considering the sampling size and good intraobserver reliability, and in the absence of other method for volume evaluation such as 3DUS and/or MRI, it is the authors' opinion that such a reference curve can be utilized in fetuses with suspected alterations in the posterior fossa. Acknowledgements The authors wish to thank Dr. Wellington de Paula Martins, from the Gynecology and Obstetrics Department of Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRP-USP), for performing the statistical analysis. REFERENCES 1. Machado A. Neuroanatomia Funcional. Belo Horizonte, MG: Atheneu; 1993. 2. Ecker JL, Shipp TD, Bromley B, et al. The sonographic diagnosis of Dandy-Walker and Dandy-Walker variant: associated findings and outcomes. Prenat Diagn. 2000;20:32832. 3. Lachmann R, Sinkovskaya E, Abuhamad A. Posterior brain in fetuses with Dandy-Walker malformation with complete agenesis of the cerebellar vermis at 11-13 weeks: a pilot study. Prenat Diagn. 2012;32:7659. 4. Patek KJ, Kline-Fath BM, Hopkin RJ, et al. Posterior fossa anomalies diagnosed with fetal MRI: associated anomalies and neurodevelopmental outcomes. Prenat Diagn. 2012;32:7582. 5. Alves CM, Araujo Júnior E, Nardozza LM, et al. Reference ranges for fetal brain fissure development on 3-dimensional sonography in the multiplanar mode. J Ultrasound Med. 2013;32:26977. 6. Bertucci E, Gindes L, Mazza V, et al. Vermian biometric parameters in the normal and abnormal fetal posterior fossa: three-dimensional sonographic study. J Ultrasound Med. 2011;30:140310. 7. Raine-Fenning NJ, Clewes JS, Kendall NR, et al. The interobserver reliability and validity of volume calculation from three-dimensional ultrasound datasets in the in vitro setting. Ultrasound Obstet Gynecol. 2003;21:28391. 8. Ruano R, Martinovic J, Dommergues M, et al. Accuracy of fetal lung volume assessed by three-dimensional sonography. Ultrasound Obstet Gynecol. 2005;26:72530. 9. Kösüs A, Kösüs N, Turhan NÖ. Are the first trimester volumetric measurements with two dimensional ultrasonography satisfactory? J Matern Fetal Neonatal Med. 2012;25:111721. 10. Kösüs N, Kösüs A, Turhan NÖ. First trimester volumetric measurements: relation with hormone levels and fetal heart rate. Arch Gynecol Obstet. 2012;286:36572. 11. Hadlock FP, Harrist RB, Martinez-Poyer J. In utero analysis of fetal growth: a sonographic weight standard. Radiology. 1991;181:12933. 12. Goldstein I, Reece EA, Pilu G, et al. Cerebellar measurements with ultrasonography in the evaluation of growth and development. Am J Obstet Gynecol. 1987;156:10659. 13. Royston P. Constructing time-specific reference ranges. Stat Med. 1991;10:67590. 14. Altman DG, Chitty LS. Charts of fetal size. 1. Methodology. Br J Obstet Gynaecol. 1994;101:2934. 15. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:30710. 16. Heard AJ, Urato AC. The isolated mildly enlarged cisterna magna in the third trimester: much ado about nothing? J Ultrasound Med. 2011;30:5913. 17. Araujo Júnior E, Guimarães Filho HA, Pires CR, et al. Validation of fetal cerebellar volume by three-dimensional ultrasonography in Brazilian population. Arch Gynecol Obstet. 2007;275:511. 18. Serhatlioglu S, Kocakoc E, Kiris A, et al. Sonographic measurement of the fetal cerebellum, cisterna magna, and cavum septum pellucidum in normal fetuses in the second and third trimesters of pregnancy. J Clin Ultrasound. 2003;31:194200. 19. Koktener A, Dilmen G, Kurt A. The cisterna magna size in normal second-trimester fetuses. J Perinat Med. 2007;35:2179. 20. Gonçalves LF, Nien JK, Espinoza J, et al. What does 2-dimensional imaging add to 3- and 4-dimensional obstetric ultrasonography? J Ultrasound Med. 2006;25:6919. 21. Araujo Júnior E, Nardozza LM, Rodrigues Pires C, et al. Comparison of two- and three-dimensional ultrasonography in lung volume measurement of normal fetuses. J Perinat Med. 2007;35:41521. 22. Araujo Júnior E, Visentainer M, Simioni C, et al. Reference values for the length and area of the fetal corpus callosum on 3-dimensional sonography using the transfrontal view. J Ultrasound Med. 2012;31:20512. 23. Wong AM, Bilaniuk LT, Zimmerman RA, et al. Prenatal MR imaging of Dandy-Walker complex: midline sagittal area analysis. Eur J Radiol. 2012;81:e2630. 1. Private Docents, Associate Professors, Obstetrics Department, Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 2. Master, Physician Assistant at Clínica Fetalmed, Curitiba, PR, Brazil 3. PhD, Associate Professor, Gynecology and Obstetrics Department, Universidade Federal do Paraná (UFPR), Curitiba, PR, Brazil 4. Private Docent, Full Professor, Obstetrics Department, Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil Mailing Address: Dr. Edward Araujo Júnior Rua Napoleão de Barros, 875, Vila Clementino São Paulo, SP, Brazil, 04024-002 E-mail: araujojred@terra.com.br Received July 2, 2013. Accepted after revision February 20, 2014. Study developed at the Obstetrics Department, Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554