Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 3 - May / June of 2014
Vol. 47 nº 3 - May / June of 2014
|
ORIGINAL ARTICLE
|
|
CT colonography: the value of this method in the view of specialists |
|
|
Autho(rs): Marcelo Longo Kierszenbaum1; Augusto Castelli von Atzingen2; Dario Ariel Tiferes3; Marcos Vinicius Alvim4, Gaspar de Jesus Lopes Filho5; Délcio Matos5; Giuseppe D'Ippolito6 |
|
|
Keywords: Computed tomography colonography; Computed tomography; Physician's practice patterns. |
|
|
Abstract: INTRODUCTION
Colorectal cancer (CRC) is the second cause of death for cancer in the United States of America(1). According to the most recent data available in Brazil, 14,180 new cases of CRC in men and 15,960 in women were estimated in 2012. Such figures correspond to an estimated risk of 15 new cases for every 100,000 men and 16 cases for every 100,000 women(2). However, it is a known fact that the screening for CRC with early detection and removal of adenomatous polyps may substantially reduce the mortality associated with CRC(3,4). It is considered that such a neoplasia has a good prognosis, provided the disease is detected(2). CRC develops from a small adenoma (< 5 mm), as a result from gene mutations, to large adenomas (> 10 mm) that generate noninvasive and invasive carcinomas(5-7). A large adenoma takes about five years to transform itself into cancer, and a small adenoma, ten to 15 years to develop malignant alterations(5). Until the present moment, fecal occult blood test, rectosigmoidoscopy, opaque enema and colonoscopy constitute the most utilized diagnostic methods to detect polyps and CRC(8). More recently (in the mid 1990s), computed tomography colonography (CTC) was introduced as a minimally invasive method developed for the diagnosis of some colorectal diseases with good acceptance by patients(9-12) and efficacy comparable to optical colonoscopy in the detection of colon polyps and CRC(13,14). As a further advantage of the method, besides being minimally invasive and sedationfree, the patient may resume his/her activities right after the procedure is completed(15,16). Recently, CTC has been offered at some university hospitals, Sistema Único de Saúde (SUS) (Unified Health System) affiliated hospitals, and at several private clinic laboratories. But it seems that CTC is still poorly requested and performed at Brazilian imaging diagnosis services due to different reasons that are still to be well established. The present study was aimed at mapping the view of specialists in the area of surgical gastroenterology and general surgery on the role played by CTC, with the purpose of depicting the scenario of its use and obtaining data to improve the accessibility and utilization of the method. MATERIALS AND METHODS The present prospective, cross-sectional and descriptive study was approved by the Committee for Ethics in Research of the authors' institution, and applied a questionnaire to specialists in surgical gastroenterology and general surgery sent by means of the Survey Monkey® survey site to members of Colégio Brasileiro de Cirurgiões (CBC) (Brazilian College of Surgeons). The site (http://www.surveymonkey.com) allows subscribers to develop and analyze online surveys. The questionnaire included 16 multiple choice questions covering items such as time of graduation of the respondent, demographic data, academic background, main work place and general knowledge about CTC (Table 1). The questionnaire was submitted by means of a link sent by e-mail to members registered at CBC under the responsibility of such a college and was anonymously answered. Neither incentive was offered in return for survey response nor was an attempt made to contact the addressees of the survey. 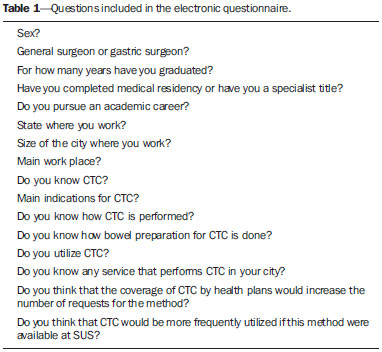 Statistical analysis The statistical analysis of all the data collected in the present study was done in a descriptive way, by calculating absolute and relative frequencies (percentages), besides the construction of bar charts. The Pearson's chi-squared test was utilized to perform the inferential analysis either to confirm or to oppose the evidences demonstrated at the descriptive analysis. The level os statistical significance corresponding to α = 5% was utilized for all the conclusions obtained by means of the inferential analysis. The data were input into worksheets Excel® 2010 for Windows® for appropriate storage. The statistical analyses were performed with the aid of the R statistical analysis software version 2.15.2. RESULTS Personal data The authors received 144 questionnaires responded by CBC members distributed as follows: 90.3% (130) men, 9.7% (14) women; 60% with less than 30 years from graduation (86/144), 77.1% (111/144) gastric surgeons, and 22.9% (33/144) general surgeons. Amongst them, 53.5% (77/144) pursued an academic career and 59.7% (86/144) developed their professional activity in cities with more than 500.000 inhabitants. The main work place was a private institution for 41.7% of the respondents, followed by 30.6% in public institutions, 18.8% in university institutions, and 9.0% in private offices (Table 2; Figures 1, 2 and 3). 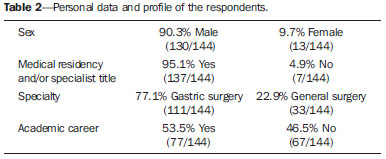 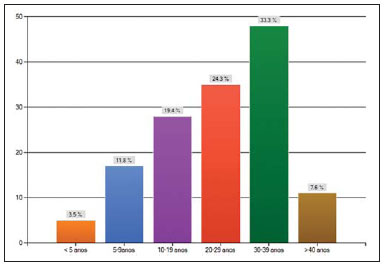 Figure 1. Time elapsed from graduation. 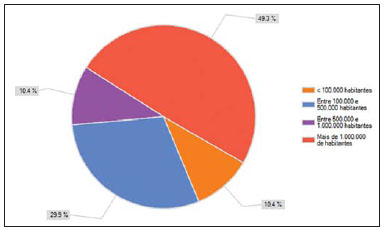 Figure 2. City where the professional works, per number of inhabitants. 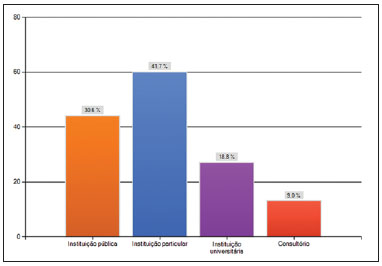 Figure 3. Distribution according the main work place of the respondents. Degree of knowledge about CTC As regards general knowledge about CTC, 84.7% of the respondents informed that knew the method, 70.8% knew how it is performed, 56.9% knew the bowel preparation utilized for the study, 31.3% utilized the method, 53.5% knew some CTC service in their city. They were also asked about the main indications for CTC. In this question, the respondent could mark as many alternatives as he/she considered correct (Table 3). The main indications for CTC included in this question were screening for CRC and incomplete colonoscopy, considered pertinent by about half of the respondents and with equal distribution between both specialties. The other indications had also a similar distribution between the two groups of specialists, except for the item "I have no opinion about it", where a prevalence was observed among in the group of general surgeons (15.3% × 27.3%; p < 0.001). It is also important to observe that only 1.4% of the respondents answered that there was no formal indication for CTC (one respondent in the group of gastric surgeons, and one in the group of general surgeons). 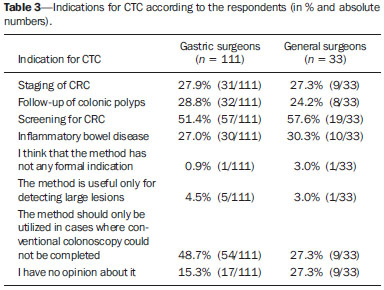 Factors limiting the use of CTC Amongst specialists, 78.5% believe that there would be a growth in requests for CTC if the method was covered by health plans, and 81.3% believe that CTC would be more frequently performed if the method were available at SUS. Cross sectional data A cross-sectional data analysis could be performed by means of tools available at the survey site. Upon the statistical analysis, the authors found the following results: - Professionals working in cities with > 500,000 inhabitants have a better knowledge about the method than those working in cities with < 500,000 inhabitants (p = 0.004) (Figure 4). 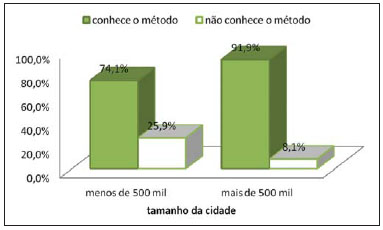 Figure 4. Size of the city × knowledge about the method. - The method is more utilized by surgeons working in cities with > 500,000 inhabitants than by those working in cities with < 500,000 inhabitants (p = 0.025) (Figure 5). 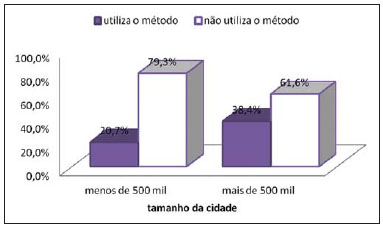 Figure 5. Size of the method × utilization of the method. - Professionals working in cities with > 500,000 inhabitants know some service that performs the method more frequently than those working in cities with < 500,000 inhabitants (p < 0.001) (Figure 6). 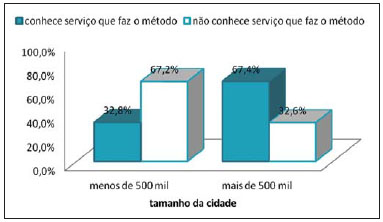 Figure 6. Size of the city × knows a service that performs CTC. - Among professionals pursuing an academic career, there is a tendency to utilize the method with greater frequency as compared with those who do not pursue such a career, but such a difference is not statistically significant (p = 0.075) (Figure 7). 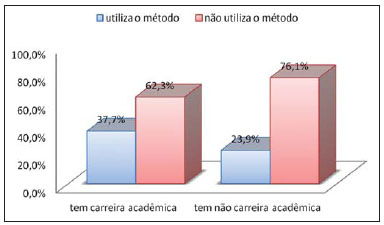 Figure 7. Academic career × utilization of the method. - Among individuals working in private or university institutions, there is a tendency to utilize the method with greater frequency as compared with those individuals working in public institutions or private offices, but such a difference is not statistically significant (p = 0.092) (Figure 8). 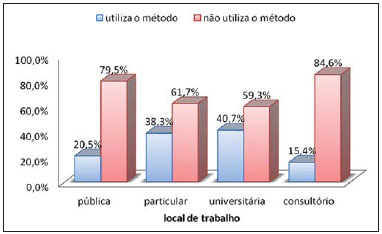 Figure 8. Work place × utilization of the method. The authors observed that the most frequent utilization of the method occurs among the respondents graduated for more than 30 years, and 37.2% out of them answered that they utilize the method. The same situation is observed in relation to the knowledge about the bowel preparation for CTC, since 64% of the respondents graduated for more than 30 years reported to have such knowledge. But, the utilization of the method and the knowledge about the bowel preparation are not associated with the time elapsed from graduation (p = 0.193 and p = 0.132, respectively - and non statistically significant). DISCUSSION Several screening program are utilized in an attempt to reduce the morbimortality of CRC. Currently, conventional colonoscopy, fecal occult blood test and carcinoembryonic antigen blood test have been the main tools utilized in the screening for CRC(3,9). A study about the view of surgeons regarding CTC is something unprecedented in Brazil and it is certainly important to establish which measures would be necessary to publicize and disseminate the utilization of the method, considering that CTC is less invasive than conventional colonoscopy, do not require sedation, and is better accepted by patients(3,10), allowing the patient to resume his/her activities right after the procedure is completed. Most respondents reported their knowledge about the method, but about half of them marked an inappropriate indication for CTC, according to the guidelines established by experts consensus. For example, according to the guidelines published by American College of Radiology, CTC should be performed for screening CRC, identifying polyps, particularly those > 5 mm, and is indicated for patients who underwent incomplete conventional colonoscopy(17). On the other hand, because CTC is performed according to a specific protocol, with bowel preparation and without using intravenous contrast injection, a priori it is not considered a method for staging, as the absence of intravenous iodinated contrast injection reduces the CTC sensitivity for detecting liver metastasis. CTC can demonstrate varied extracolonic lesions(18), including possible metastases, but cannot be considered a method for disease staging. For such a purpose, a further contrast-enhanced phase must be added(19), which is not routinely performed in CTC. About 50% of surgeons participating in the study indicated that CRC staging would be an indication for CTC, which does not correspond to the original potential of the method. An appropriate CTC requires distension of the colon by means of inflation with gas inserted, either mechanically or manually, through the rectum; for this reason, the use of CTC in cases of inflammatory bowel disease may lead to complications such as bowel perforation and peritonitis, particularly in patients with active disease(20,21). For these reasons, CTC is relatively contraindicated in this specific group of patients and if for some reason the procedure must be performed, it should be done according to a protocol and under specific measures(22). In this context, about one third of the surgeons answered that they believe that CTC could be indicated to investigate inflammatory bowel disease, which is at least a questionable indication. Specialists working in cities with > 500,000 inhabitants know and utilize the method more frequently. Such a fact is compatible with the Brazilian reality, considering that larger cities have a tendency to have easier access to diagnostic imaging methods and to skilled professionals to perform and interpret specific studies(23). As expected, in the present study the authors could observe that professionals pursuing an academic career and working at university hospitals know and utilize CTC with greater frequency, probably because they are in closer contact with modern diagnostic methods and more exposed to innovation, besides being in contact with peer radiologists who are familiar with the method. In a referral to the site of Agência Nacional de Saúde (National Health Agency) (www.ans.gov.br), the authors observed that the procedure is still to be included in the minimum list of procedures that must be covered by health plans(24). Like the respondents in the present study, the authors believe that the number of procedures and professionals interested in requesting and performing the method will increase as CTC is included in the list of basic procedures to be covered by health plans. Considering that CTC is an excellent method for screening CRC, with good acceptance by patients and increasing availability in Brazil, which would be the true reason behind the poor utilization of CTC in our country? In order to answer such a question, the authors have created the mentioned questionnaire and, based on the responses they could make some observations. They have found that many professionals involved with the management of patients in their daily routines do know the method and a place in their cities where the procedure is performed. However, only about 30% of such professionals utilize the method. The authors observed that factors such as involvement in academic career, work place and size of the city are directly associated with the knowledge about CTC and, consequently, with the indication and performance of CTC. For a greater dissemination of CTC in Brazil, a more intensive effort would be necessary to inform requesting physicians about indications, limitations and advantages of the method (as compared with the conventional colonoscopy), in addition to an effort of entities representing the professionals (such as Colégio Brasileiro de Radiologia e Diagnóstico por Imagem), towards including CTC in the list of procedures covered by health plans and in the unified diagnostic procedures table of SUS. The present study has some limitations. The questionnaires were sent by electronic means and maybe many of them have not been answered, reducing the size of the study sample. The authors could not know the exact number of the CBC member who received the questionnaire. Considering that CTC is a relatively new method in Brazil, maybe some professionals have quit answering the questionnaire simply because they did not know the method, despite the fact that their participation was anonymous. The present study sample could be larger, but the statistical analysis of specific variables has demonstrated that the sample was sufficient and the obtained data were reliable. Additionally, the data were not analyzed per region, so the generalization might lead to inaccuracy. A higher number of respondents proportionally distributed throughout the whole Brazilian territory would be necessary to obtain more reliable data applicable per studied region, hence the objective of the questionnaire in determining the respondent's state of origin. But this objective was not successfully achieved because of the limited number of responses coming from some Brazilian regions. Even dividing the respondents according their region of origin, the figures obtained from the Northern and Northeastern regions were not sufficient to allow for a statistical analysis. Such analysis might be part of a further investigation. On the other hand, as the authors classified the questionnaires according to the number of inhabitants in the cities of the respondents, obtaining significant results, they believe that such a limitation was partially bypassed. Finally another limitation of the present study was related to the fact that the authors have not specifically investigated a group of surgeons specialized in coloproctology and conventional colonoscopy. Such data might confirm the authors' expectations, i.e., that a coloproctologist has a deeper knowledge about CTC as compared with general gastric surgeons, and that the fact that they perform conventional colonoscopy might in some way negatively influence in the option for performing an alternative diagnostic method. The authors have not found any evidence in the literature confirming such assumptions. On the other hand, the present study was not aimed at demonstrating the existence of a cause/effect relation between the control over the conventional colonoscopic technique and the knowledge and utilization of CTC. Finally, as the authors depicted the profile and the view of specialists in relation to the use of CTC, they have found out that the method, although still poorly utilized in Brazil, is widely known, particularly in large urban centers and in the academic environment. A project of divulgation of CTC in association with an effort to include this method in the diagnostic procedures tables, may allow for a greater contribution to the screening for CRC, so CTC becomes a relevant tool to reduce the disease morbimortality. REFERENCES 1. Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277-300. 2. Brasil. Ministério da Saúde. Instituto Nacional de Câncer. Estimativa 2012: incidência de câncer no Brasil. Rio de Janeiro, RJ: INCA; 2012. 3. Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58:130-60. 4. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale - update based on new evidence. Gastroenterology. 2003;124:544-60. 5. Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251-70. 6. Aldridge AJ, Simson JN. Histological assessment of colorectal adenomas by size. Are polyps less than 10 mm in size clinically important? Eur J Surg. 2001;167:777-81. 7. Winawer SJ. Natural history of colorectal cancer. Am J Med. 1999;106(1A):3S-6S. 8. Pickhardt PJ, Hassan C, Halligan S, et al. Colorectal cancer: CT colonography and colonoscopy for detection - systematic review and meta-analysis. Radiology. 2011;259:393-405. 9. Maia MVAS, von Atzingen AC, Tiferes DA, et al. Preferência do paciente no rastreamento do câncer colorretal: uma comparação entre colonografia por tomografia computadorizada e colonoscopia. Radiol Bras. 2012;45:24-8. 10. von Wagner C, Ghanouni A, Halligan S, et al. Acceptability and psychologic consequences of CT colonography compared with those of colonoscopy: results from a multicenter randomized controlled trial of symptomatic patients. Radiology. 2012;263:723-31. 11. Pooler BD, Baumel MJ, Cash BD, et al. Screening CT colonography: multicenter survey of patient experience, preference, and potential impact on adherence. AJR Am J Roentgenol. 2012;198:1361-6. 12. von Wagner C, Knight K, Halligan S, et al. Patient experiences of colonoscopy, barium enema and CT colonography: a qualitative study. Br J Radiol. 2009;82:13-9. 13. Graser A, Stieber P, Nagel D, et al. Comparison of CT colonography, colonoscopy, sigmoidoscopy and faecal occult blood tests for the detection of advanced adenoma in an average risk population. Gut. 2009;58:241-8. 14. Regge D, Laudi C, Galatola G, et al. Diagnostic accuracy of computed tomographic colonography for the detection of advanced neoplasia in individuals at increased risk of colorectal cancer. JAMA. 2009;301:2453-61. 15. Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003;349:2191-200. 16. von Atzingen AC, Tiferes DA, Matsumoto CA, et al. Aspectos comuns e pseudolesões na colonografia por tomografia computadorizada: ensaio iconográfico. Radiol Bras. 2012;45:160-6. 17. American College of Radiology. ACR practice guideline for the performance of computed tomography (CT) colonography in adults. Reston, VA: American College of Radiology; 2009. 18. Veerappan GR, Ally MR, Choi JH, et al. Extracolonic findings on CT colonography increases yield of colorectal cancer screening. AJR Am J Roentgenol. 2010;195:677-86. 19. Chung DJ, Huh KC, Choi WJ, et al. CT colonography using 16-MDCT in the evaluation of colorectal cancer. AJR Am J Roentgenol. 2005;184:98-103. 20. Berrington de Gonzalez AB, Kim KP, Yee J. CT colonography: perforation rates and potential radiation risks. Gastrointest Endosc Clin N Am. 2010;20:279-91. 21. Burling D, Halligan S, Slater A, et al. Potentially serious adverse events at CT colonography in symptomatic patients: national survey of the United Kingdom. Radiology. 2006;239:464-71. 22. Mang T, Maier A, Plank C, et al. Pitfalls in multi-detector row CT colonography: a systematic approach. Radiographics. 2007;27:431-54. 23. Conselho Federal de Medicina, Conselho Regional de Medicina do Estado de São Paulo. Demografia médica no Brasil. Volume 2 - Cenários e indicadores de distribuição. Relatório de pesquisa. São Paulo, SP: CFM/CREMESP; 2013. [acessado em 27 de maio de 2013]. Disponível em: http://portal.cfm.org.br/images/stories/pdf/demografiamedicanobrasil_vol2.pdf. 24. Brasil. Ministério da Saúde. Agência Nacional de Saúde Suplementar. Relatório de pesquisa. Brasilia, DF: ANS; 2013. [acessado em 27 de maio de 2013]. Disponível em: http://www.ans.gov.br/planos-de-saude-e-operadoras/espaco-do consumidor/1149-verificar-cobertura-de-planoEstimativa. 1. MD, Radiologist, Department of Imaging Diagnosis, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 2. PhD, MD, Radiologist, Department of Imaging Diagnosis, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 3. PhD, MD, Radiologist, Department of Imaging Diagnosis, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), MD, Laboratório Fleury-São Paulo, São Paulo, SP, Brazil 4. MD, Radiologist, Department of Imaging Diagnosis, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 5. Full Professors, Division of Surgical Gastroenterology, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil 6. Professor, Department of Imaging Diagnosis, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), MD, Laboratório Fleury-São Paulo, São Paulo, SP, Brazil Mailing Address: Dr. Giuseppe D'Ippolito Departamento de Diagnóstico por Imagem - EPM-Unifesp Rua Napoleão de Barros, 800, Vila Clementino São Paulo, SP, Brazil, 04024-002 E-mail: giuseppe_dr@uol.com.br Received June 21, 2013. Accepted after revision January 8, 2014. Study developed at Department of Imaging Diagnosis and at the Division of Surgical Gastroenterology, Escola Paulista de Medicina - Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554