Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 3 - May / June of 2014
Vol. 47 nº 3 - May / June of 2014
|
CASE REPORT
|
|
Cloverleaf skull syndrome: case report |
|
|
Autho(rs): Junio Marcos Fonseca1; Luciana Mendes Araújo Borém2 |
|
|
Keywords: Syndrome; Malformation; Computed tomography. |
|
|
Abstract: INTRODUCTION
Cloverleaf skull syndrome is an abnormal configuration of the calvaria classified as craniosynostosis, consisting of premature ossification of cranial sutures. It is a deformity characterized by a remarkable enlargement of the head, with a trilobed configuration of the frontal view, resembling a threeleaved clover(1). This abnormality occurs as a result from a severe alteration in the development of the skull, with premature synostosis of some cranial sutures(1), most commonly the coronal and lambdoid sutures(2), in association with hydrocephalus, leading to a marked bulging of the head in the region of the anterior fontanel and laterally in the temporal regions, with the typical appearance of a "cloverleaf"(1). Syndromic and nonsyndromic presentations have been reported. Because of the anomalies both in the calvaria and in the skull base and face, this is one of the craniosynostoses currently requiring the most complex multidisciplinary approach(1). The first report about such a syndrome in the literature occurred in 1973 and, over the years only some tens of cases have been documented worldwide(3). The present report describes a case of a severe craniofacial condition that is known as "cloverleaf skull syndrome". CASE REPORT A female patient born from Cesarean section on January 4, 2011, weighting 3,815 g and Apgar 7 and 8 at the first and fifth minute of life, respectively. At physical examination multiple malformations were observed, with altered craniofacial configuration, low ear implantation, hypertelorism, exophthalmos, omphalocele and polydactyly (Figure 1). Chest radiography demonstrated dextrocardia (Figure 2), and computed tomography demonstrated abnormal configuration of the calvaria, with the typical trilobed "cloverleaf" aspect, bulging of the middle cranial fossae and dilatation of the ventricular system. Signs of closure of sagittal, coronal and lambdoid sutures were also observed (Figure 3). The patient presented cardiorespiratory arrest episodes, progressing to death on January 7, 2011.  Figure 1. A: Demonstration of typical craniofacial alterations. B: Syndactyly (arrow). 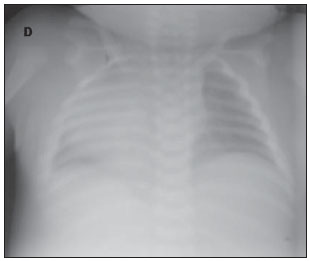 Figure 2. Chest radiography demonstrating dextrocardia. 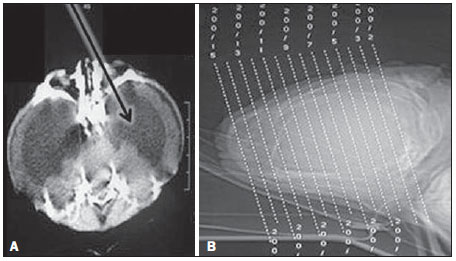 Figure 3. A: Trilobed aspect of the skull, with hydrocephalus and bulging of the middle fossae (arrow). B: Scout demonstrating a marked enlargement of the skull in the region of the anterior fontanel. DISCUSSION Cloverleaf skull syndrome is a rare presentation of craniosynostosis with clinical features consisting in trilobed skull, exophthalmos, low ear implantation and upper airway. Hydrocephalus is also a common finding, despite the multifactorial nature of such an abnormality(4). It is a congenital anomaly that may be present as an isolated defect, but generally is classified as dysostotic syndromes such as achondroplasia, craniofacial dysostosis (Crouzon syndrome), Apert or Pfeiffer syndromes(2). Until 1981, only 30 cases had been published in the literature, the first of them in 1973, in the ophthalmic literature(3). The precise etiopathogenesis of this syndrome is still to be completely known(3), with theories involving altered membranous-osseous and/or endochondral ossification, generalized chondrodysplastic process(2), and a possible vascular origin associated with the abnormal osteoclastic resorption(5). Recently, genetic investigations have contributed to advances in the understanding of the molecular basis of some craniosynostosis syndromes, highlighting mutations in the genes FGFR1, FGFR2, FGFR3, TWIST and MSX2(6). The diagnosis of such a syndrome can be made in the prenatal period by means of ultrasonography, which detects the altered cranial morphology and hydrocephalus. Traditionally, the diagnosis occurs during routine prenatal followup at the second gestational trimester. However, with the increasing use of obstetric ultrasonography at the first gestational trimester, such alterations may be detected increasingly earlier over the gestation(7). After birth, as an abnormal configuration of the calvaria is detected, a radiological evaluation is required to characterize the deformity and guide the corrective surgical procedure. There is a significant improvement in the prognosis of affected children in cases where the diagnosis and the surgical intervention occur as early as possible. Computed tomography with three-dimensional reconstruction contributes to the assessment of craniofacial bone deformities and associated intracranial alterations, demonstrating to be a useful tool to define the prognosis and for the surgical planning(8). The present case was not classified into any specific syndrome category, and the cardiorespiratory instability hindered the attempts of surgical intervention. The early death of the infant demonstrates how the association with malformations may worsen the prognosis of this condition. Despite the unfavorable outcome of many cases, advances in surgical, anesthetic and intensive care techniques have transformed a condition previously considered untreatable into a potentially treatable condition, with acceptable neurological and aesthetic results(2). The relevance of the imaging diagnosis and characterization of this syndrome, particularly in the prenatal period, is highlighted in order to allow for the planning and institution of the treatment as earlier as possible. REFERENCES 1. Iannaccone G, Gerlini G. The so-called "cloverleaf skull syndrome". A report of three cases with a discussion of its relationships with thanatophoric dwarfism and the craniostenoses. Pediat Radiol. 1974;2:175-84. 2. Manjila S, Chim H, Eisele S, et al. History of the Kleeblattschädel deformity: origin of concepts and evolution of management in the past 50 years. Neurosurg Focus. 2010;29:E7. 3. Ghose S, Mehta U. The Kleeblattschadel (cloverleaf skull) syndrome. Indian J Ophthalmol. 1986;34:61-6. 4. Ito S, Matsui K, Ohsaki E, et al. A cloverleaf skull syndrome probably of Beare-Stevenson type associated with Chiari malformation. Brain Dev. 1996;18:307-11. 5. Dambrain R, Freund M, Verellen G, et al. Considerations about the cloverleaf skull. J Craniofac Genet Dev Biol. 1987;7:387-401. 6. Arduino-Meirelles AP, Lacerda CBF, Gil-da-Silva-Lopes VL. Aspectos sobre desenvolvimento de linguagem oral em craniossinostoses sindrômicas. Pró-Fono. 2006;18:213-20. 7. Chitty LS, Khalil A, Barrett AN, et al. Safe, accurate, prenatal diagnosis of thanatophoric dysplasia using ultrasound and free fetal DNA. Prenatal Diagn. 2013;33:416-23. 8. Trad CS, Rosique RG. Craniossinostoses primárias: ensaio iconográfico. Radiol Bras. 2005;38:377-80. 1. Biomedicine Post-graduate, Technical Coordinator, Imaging Division of Fundação Dilson Godinho, Montes Claros, MG, Brazil 2. Master, Fellow PhD degree, MD, Radiologist at Hospital Santa Casa de Montes Claros, Montes Claros, MG, Brazil Mailing Address: Junio Marcos Fonseca Rua Guiana Francesa, 200, Bairro João Alves Montes Claros, MG, Brazil, 39402-307 E-mail: juniofonseca@hotmail.com Received January 28, 2013. Accepted after revision August 12, 2013. Study developed at Hospital Santa Casa de Montes Claros, Montes Claros, MG, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554