Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 46 nº 1 - Jan. /Feb. of 2013
Vol. 46 nº 1 - Jan. /Feb. of 2013
|
ORIGINAL ARTICLE
|
|
Detection of abdominal aortic calcification by densitometry |
|
|
Autho(rs): Osvaldo Sampaio Netto1; Caroline Louise Hasselmann2; Evandro Cesar Vidal Osterne3; Otoni Moreira Gomes4 |
|
|
Keywords: Atherosclerosis; Abdominal aorta; Densitometry. |
|
|
Abstract: INTRODUCTION
The densitometry apparatuses were introduced in the 1960's with the purpose of evaluating bone density. Initially the resolution was low and the scan time was long(1). Over the last decades densitometry has undergone huge developments, with increased resolution while maintaining low dose of radiation exposure, becoming the gold standard for bone density evaluation(2,3). By the end of the 20th century, such developments enabled the introduction of apparatuses capable of evaluating the presence of vertebral fractures through the measurement of height and diameter of lumbar and thoracic vertebrae(4). With such increased resolution with a low radiation dose, the utilization of densitometers for detecting calcification in non-osseous structures has been proposed. The evaluation of abdominal aortic calcification for investigation of atherosclerosis in asymptomatic patients is promising and can be performed with the same technique utilized for evaluation of vertebral fractures. Currently, the evaluation of abdominal aortic calcification may be performed with lateral lumbar spine radiography or by means of computed tomography. Radiography is the simplest method available for evaluation of the aorta, particularly in the screening of asymptomatic patients with risk factors for development of atherosclerosis. Aortography, computed tomography and magnetic resonance imaging can be performed in symptomatic patients to evaluate aortic aneurysms and acute aortic obstruction(5,6). Wilson et al.(7), in a study published in 2001, observed the presence of abdominal aortic calcification by means of lateral spine radiography as a predictor of cardiovascular disorders in approximately 2,500 individuals, between the years of 1967 and 1989, obtaining a relative risk of 1.33 for men and 1.25 for women. A study published by Schousboe et al.(8)in 2006 suggests that during the performance of vertebral fracture assessment (VFA), it is possible to include the lumbar spine and the soft tissue region anterior to the lumbar spine on a single image, allowing the detection of abdominal aortic calcification, and thus, with the same diagnostic study, detect the risk factors for the two most prevalent disorders in public health - osteoporosis and cardiovascular diseases. The present study is aimed at analyzing the accuracy of densitometry in the detection of abdominal aortic calcification as compared with spine radiography. MATERIALS AND METHODS The research project on detection of abdominal aortic calcification by means of lateral spine densitometry was approved by the Committee for Ethics in Research of Universidade Católica de Brasília on May 15, 2008, official letter CEP/UCB No. 055/2008. This was a prospective study, whose sample consisted of the first 80 individuals from both sexes, who met the inclusion/exclusion criteria, 50 of them with diagnosis of abdominal aortic calcification, and 30 without such diagnosis, who agreed to and signed a term of free and informed consent. Volunteers were selected according to the following inclusion criteria: patients with radiological diagnosis of abdominal aortic calcification, or elderly individuals with a history of heart disease or increased triglycerides/cholesterol levels either with or without confirmed radiological diagnosis of abdominal aortic calcification. The exclusion criterion which hindered the participation in the study was the presence of metal prosthesis in the thoracic or lumbar spine. Bone densitometry was performed a single time for each participant, with a Discovery W model Hologic® densitometer, with fan beam technology, emitting 100 and 140 kV X-rays with 128 detectors and 2 mm resolution(9). The densitometry scans were performed in lateral view of the vertebral spine, with the patients wearing metal-free clothing and positioned in right lateral decubitus; and lasted approximately 45 seconds. The patients were requested to fast for four hours before the scan. With this method, the patient absorbed radiation dose is 25 µSv(9). The reports were issued by a physician accredited by Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (Brazilian College of Radiology and Imaging Diagnosis) and by Sociedade Brasileira de Densitometria Clínica (Brazilian Society of Clinical Densitometry), with an experience of more than 15 years in densitometry. The statistical analysis of data regarding sample categorization, contingency table and qualitative test of kappa correlation was performed with the softwares Microsoft Office Excel 2007® and IBM SPSS Statistics 19.0®. RESULTS In the period between May, 2008 and June, 2010, 80 densitometry scans were performed to evaluate abdominal aortic calcification in 50 patients previously diagnosed with abdominal aortic calcification and in 30 patients without the condition. The sample comprised 21 male and 59 female patients and, among them 12 men and 38 women had previously been diagnosed with abdominal aortic calcification. The mean age of the patients with abdominal aortic calcification was 74.56 ± 10.55 years, and in the case of the patients without calcification the mean age was 68.40 ± 10.80 years. Mean body mass index (BMI) was 28.94 ± 6.06 kg/m2 in the patients with calcification and 26.84 ± 4.11 kg/m2 in the patients without the condition. In the group of 30 patients without abdominal aortic calcification, the densitometry confirmed the absence of the condition. In the group of 50 patients previously diagnosed with abdominal aortic calcification, densitometry identified 47 patients with the disorder. In the examples on Figure 1, the presence of abdominal aortic calcification can be observed at the densitometric image, anteriorly to three or more lumbar vertebrae. 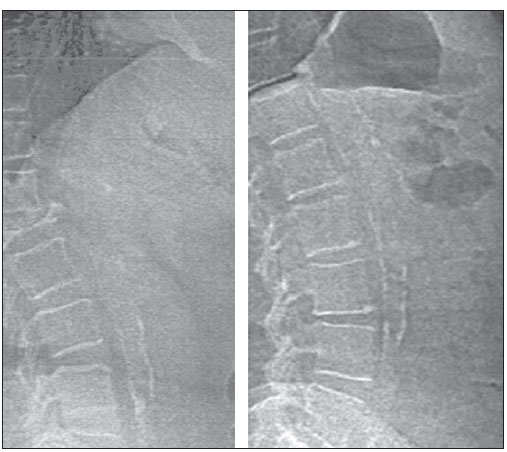 Figure 1. Densitometry results demonstrating the presence of abdominal aortic calcification in the frontal region of three or more lumbar vertebrae. By means of statistical analysis of a contingency table for evaluation of diagnostic studies, the authors observed that the investigation of abdominal aortic calcification by means of densitometry presented 94.0% sensitivity, 100% specificity, 100% positive predictive value, 90.9% negative predictive value and 96.3% accuracy, as compared with the radiological diagnosis. As the densitometric results were analyzed for the two groups, with positive and negative radiological diagnosis of abdominal aortic calcification, the statistical kappa test was applied in order to analyze the qualitative correlation of the results, with a kappa index of 0.922, corresponding to a statistical significance level of p < 0.01. DISCUSSION The presence of atherosclerosis is one of the main triggering factors for cardiovascular diseases(10), thus the importance of developing methods to allow an early detection of the development of atherosclerosis. Atherosclerosis is a systemic disease that may simultaneously involve several arteries. As the development of atherosclerosis is investigated, one can find that generally such a disease begins in large elastic arteries and then affects large and medium caliper muscular arteries(11). The Rotterdam Coronary Calcification Study developed with 2,013 individuals with ages ≥ 55 years, demonstrates a strong association between the presence of coronary calcifications and abdominal aortic calcification(12). It is important to highlight the natural history of the development of atherosclerosis. The major focus of investigation of atherosclerosis has been the coronary and carotid arteries, while abdominal aortic calcification precedes the compromising of those arteries(7,12). Hollander et al.(13), analyzing the cohort of the Rotterdam Coronary Calcification Study, have found that abdominal aortic calcification and presence of atherosclerosis in the carotid arteries represent strong predictors of incidence of stroke, with a relative risk of 1.89 and 2.23, respectively. In a study published in 2010, Bolland et al.(14) analyzed abdominal aortic calcification by means of lateral abdominal radiography, and estimated that the presence of such condition increases the risk for acute myocardial infarction independently in men (odds ratio of 5.32, with p = 0.04) and in women (odds ratio of 2.30, with p = 0.007). The analysis in women demonstrated that abdominal aortic calcification is an independent factor for severe cardiovascular events (acute myocardial infarction, stroke or sudden death), with an odds ratio of 1.74, with p = 0,007. Rodondi et al.(15), in a study published in 2007, followed-up 2,056 women aged ≥ 65, diagnosed with abdominal aortic calcification by means of lateral spine radiography, over a 13-year period, in order to investigate the risk for cardiovascular death. The authors concluded that abdominal aortic calcification posed a risk of 1.18 for cardiovascular mortality and mainly a risk of 1.53 for coronary artery disease. Thus, the investigation of abdominal aortic calcification allows an earlier diagnosis of atherosclerosis and, consequently the treatment of the condition before the compromising of the coronary and carotid arteries. Besides being a predictive factor for cardiovascular disease, abdominal aortic calcification is also a predictive factor for cerebral vascular disease and may cause aortic aneurysm and acute aortic obstruction(7,16-18). The diagnostic investigation in cases of aneurysm and acute obstruction is performed by means of computed tomography and magnetic resonance imaging, which provide better visualization and measurement of the atherosclerotic plaque(5). For screening in asymptomatic patients, the technique utilized is lateral lumbar spine radiography, like in the studies developed by Framingham(7) and in the Rotterdam Coronary Calcification Study(12). The main limiting factor for routine performance of lateral lumbar spine radiography in asymptomatic patients is the radiation dose to which the patient is exposed, of approximately 700-800 µSv(3,19-21). The proposal for utilization of densitometry equipment came after the development of the method for morphometric evaluation of the lumbar spine employed in the investigation of vertebral fractures. The investigation of abdominal aortic calcification is performed with the same technique utilized for VFA, with the main advantage of being a technique with a low radiation dose for the patients. In the current apparatuses, such dose is approximately 25 µSv(9,22). Additionally, there are other advantages such as the fact that the scan takes only 45 seconds to be completed and the minimum preparation required from the patients: four-hour fasting before the scan and wearing metal-free clothing. In the characterization of the present study sample, the authors observed that, despite the predominance of female patients, a similar distribution of male and female patients occurred in the two groups. In the group of patients with abdominal aortic calcification, 24% were men and 76% were women, while in the group of patients without abdominal aortic calcification, 30% were men and 70% were women. As regards age, the groups were also similar, with mean ages of 74.56 ± 10.55 years and 68.40 ± 10.80 years in the groups with and without calcification, respectively. In both groups the lowest ages were around 50 years and the highest ages were above 90 years. The BMI also presented similar distribution in both groups, with mean values of 28.94 ± 6.06 kg/m2 in those patients with abdominal aortic calcification and 26.84 ± 4.11 kg/m2 in those patients without the condition. Such considerations regarding age and BMI are relevant as the physical capacity of the patient to sustain the positioning (right lateral decubitus) required for the performance of the scan for the duration of the procedure. In the group of 50 patients with radiological diagnosis of abdominal aortic calcification, lateral lumbar spine densitometry detected the presence of calcification in 47 patients. In three patients the authors did not found the presence of abdominal aortic calcification. However, multiple gas bubbles could be observed, including bubbles in the anterior region of the vertebral spine, which could be possibly the cause for non visualization of the calcification, a fact that may suggest the need for longer fasting before densitometry. In the present study, four-hour fasting before the scan was adopted. In the evaluation of the patients whose radiological diagnoses were negative for abdominal aortic calcification, densitometry was also negative in all patients. The statistical comparison between densitometry and radiography demonstrates that both methods are similar in the identification of abdominal aortic calcification. Values of 100% were obtained for specificity and positive predictive value - high values as compared with sensitivity (94%), negative predictive value (90.9%) and accuracy (96.3%). The equivalence between the two methods in the qualitative evaluation of presence or not of abdominal aortic calcification is corroborated by the kappa correlation index of 0.922. Both radiological investigation and the proposed utilization of densitometry are aimed at investigating the asymptomatic patient, increasing the possibility of preventing the development of atherosclerosis before it affects the carotid or the coronary arteries. The utilization of investigation by bone densitometry is faced the limiting factor of not being capable of measuring the atherosclerotic plaque. It is important to instruct the patient to fast for at least four hours before the scan, in order to avoid the presence of intestinal gas bubbles which might impair the correct analysis of the image. The authors have observed that both methods present a statistically similar accuracy, and that the difference that should be taken into consideration is radiation dose to which the patient is exposed: 700-800 µSv for radiography and 20-40 µSv(3,9,19-22)for densitometry. CONCLUSION Over the past decades, the investigation of abdominal aortic calcification in asymptomatic patients has been performed by means of conventional radiograph. Analyzing this investigation using densitometry apparatuses, one observes that the results obtained by densitometry are statistically equivalent. Thus, the authors suggest that densitometry equipment can be utilized to investigate abdominal aortic calcification. REFERENCES 1. Cameron JR, Sorenson J. Measurement of bone mineral in vivo: an improved method. Science. 1963;142:230-2. 2. Glüer CC, Steiger P, Selvidge R, et al. Comparative assessment of dual-photon absorptiometry and dual-energy radiography. Radiology. 1990;174:223-8. 3. World Health Organization. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series No 843. WHO Study Group. Geneva, Switzerland: WHO; 1994. 4. Vokes T, Bachman D, Baim S, et al. Vertebral fracture assessment: the 2005 ISCD Official Positions. J Clin Densitom. 2006;9:37-46. 5. Isselbacher EM. Aortic diseases. In: Libby P, Bonow RO, Mann DL, et al., editors. Braunwald's Heart disease: a textbook of cardiovascular medicine. 8th ed. Philadelphia, PA: Elsevier; 2007. p. 606-20 6. Elfteriades JA, Olin JW, Halperin JL. Diseases of the aorta. In: Fuster V, O'Rourke RA, Walsh RA, et al., editors. Hurst's The heart. 12th ed. New York, NY: McGraw-Hill; 2008. p. 2305-28 7. Wilson PW, Kauppila LI, O'Donnell CJ, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation. 2001;103:1529-34. 8. Schousboe JT, Wilson KE, Kiel DP. Detection of abdominal aortic calcification with lateral spine imaging using DXA. J Clin Densitom. 2006;9:302-8. 9. Hologic. QDR® series X-ray bone densitometers. Technical specifications manual. Bedford, MA: Hologic Inc.; 2006. 10. Strong JP. Natural history and risk factors for early human atherogenesis. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. Clin Chem. 1995;41:134-8. 11. Mitchell RN, Schoen FJ. Blood vessels. In: Kumar V, Abbas AK, Fausto N, et al., editors. Robbins and Cotran Pathologic basis of disease. 8th ed. Philadelphia, PA: Elsevier; 2009. p. 508-18. 12. Oei HH, Vliegenthart R, Hak AE, et al. The association between coronary calcification assessed by electron beam computed tomography and measures of extracoronary atherosclerosis: the Rotterdam Coronary Calcification Study. J Am Coll Cardiol. 2002;39:1745-51. 13. Hollander M, Hak AE, Koudstaal PJ, et al. Comparison between measures of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke. 2003;34:2367-72. 14. Bolland MJ, Wang TK, van Pelt NC, et al. Abdominal aortic calcification on vertebral morphometry images predicts incident myocardial infarction. J Bone Miner Res. 2010;25:505-12. 15. Rodondi N, Taylor BC, Bauer DC, et al. Association between aortic calcification and total and cardiovascular mortality in older women. J Intern Med. 2007;261:238-44. 16. Witteman JCM, Kok FJ, van Saase JLC, et al. Aortic calcification as a predictor of cardiovascular mortality. Lancet. 1986;2:1120-2. 17. Witteman JCM, Kannel WB, Wolf PA, et al. Aortic calcified plaques and cardiovascular disease (the Framingham Study). Am J Cardiol. 1990;66:1060-4. 18. Auerbach O, Garfinkel L. Atherosclerosis and aneurysm of aorta in relation to smoking habits and age. Chest. 1980;78:805-9. 19. Huda W, Morin RL. Patient doses in bone mineral densitometry. Br J Radiol. 1996;69:422-5. 20. Kalender WA. Effective dose values in bone mineral measurements by photon absorptiometry and computed tomography. Osteoporos Int. 1992;2:82-7. 21. Szejnfeld VA, Heymann RE. Avaliação da massa óssea por DXA. In: Anijar JR. Densitometria óssea na prática médica. 1ª ed. São Paulo, SP: Sarvier; 2003. p. 17-26. 22. Damiano J, Kolta S, Porcher R, et al. Diagnosis of vertebral fractures by vertebral fracture assessment. J Clin Densitom. 2006;9:66-71. 1. PhD, Nuclear Physician, Professor at Universidade Católica de Brasília (UCB), Brasília, DF, Brazil. 2. MD, Universidade Católica de Brasília (UCB), Brasília, DF, Brazil. 3. PhD, Interventional Cardiologist, Professor at Universidade Católica de Brasília (UCB), Brasília, DF, Orienting Professor at Fundação Cardiovascular São Francisco de Assis (FCSFA), Belo Horizonte, MG, Brazil. 4. PhD, Cardiovascular Surgeon, Professor at Universidade Federal de Minas Gerais (UFMG), Orienting Professor at Fundação Cardiovascular São Francisco de Assis (FCSFA), Belo Horizonte, MG, Brazil. Mailing Address: Dr. Osvaldo Sampaio Netto SHLN 116, Ed. Multiclínicas, sala 14, Asa Norte Brasília, DF, Brazil, 70770-560 E-mail: osvsamp@gmail.com Received August 2, 2012. Accepted after revision December 7, 2012. * Study developed at Universidade Católica de Brasília (UCB), Brasília, DF, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554