Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 6 - Nov. / Dec. of 2012
Vol. 45 nº 6 - Nov. / Dec. of 2012
|
ORIGINAL ARTICLE
|
|
Dosimetry in abdominal imaging by 6-slice computed tomography |
|
|
Autho(rs): Sónia Isabel Rodrigues1; António Fernando Abrantes2; Luis Pedro Ribeiro3; Rui Pedro Pereira Almeida |
|
|
Keywords: Computed tomography; Dosimetry; ALARA; CTDI; Optimization; Body mass index. |
|
|
Abstract: INTRODUCTION
Computed tomography (CT) was introduced in medical imaging in 1972 and has quickly developed both in terms of technical performance and clinical utilization. Spiral CT and, in particular, the latest generation of detectors with multislice capability have allowed for improvement in acquisition time and in imaging quality, which results in information with a high degree of reliability, depicting all parts of the human body, without artifacts caused by peristaltic and respiratory movements(1). The range of applications has increased, for example by means of CT angiography, virtual endoscopy, multiphase contrast-enhanced studies and multiplanar volume reconstruction(2,3). With increasing number of applications, the relative contribution of CT to the dose resulting from medical procedures has proportionally increased(4). Due to the fact that such doses are relatively high, they end up having a significant impact on the doses on the population, thus the evaluation of medical exposure in CT studies is of particular relevance(5). In 2007, in USA, the estimated effective collective dose for CT examinations, even after adjustment for the population size, was 440,000 Sv as compared with 18,000 Sv in the United Kingdom, with the radiation dose attributed to CT being 0.35 mSv per capita in the United Kingdom population and 1.5 mSv in the USA(5). One of the biological effects of ionizing radiation is cancer induction. Recent studies have concluded that there is a probability of 1 in 1,000 of cancer induction for a 10 mSv exposure. In children, such a fact is even more critical, as the occurrence of cancer has a longer time to manifest(6). For all those reasons, dose reduction in CT is extremely important, with assurance of appropriate justification for all studies, as well as the utilization of appropriate technical parameters, equipment quality control and utilization of the lowest possible diagnosis reference levels(1). On account of geometry and application of the CT technique, such a method comprises a set of quantities to quantify the exposure to radiation, namely: computed tomography dose index (CTDI), doselength product (DLP) and effective dose(7). In CT, dose measurements may be performed by means of the Monte Carlo simulation or by means of dosimeters, such as radiophotographic films, thermoluminescent dosimeters and ionization chambers. Thus, following up on the previously mentioned facts, the present study was aimed at determining the received dose values at abdominal CT examinations and the relationship of such values with the anthropometric characteristics of the patient, namely sex, age, body mass index (BMI), height, and abdominal perimeter. The development of the present investigation is considered to be of great relevance, as the abdominal studies are the most frequently performed among all CT studies, and also those which most contribute to the received radiation dose. As a function of the obtained results, the present study is also aimed at presenting a set of recommendations for dose optimization in such type of examination. MATERIALS AND METHODS The target population of the present study consisted of patients who underwent abdominal CT examinations in the Imaging Service of Hospital de Faro, EPE, located in Southern Portugal. The sample included 100 physically able patients (44 women and 56 men) with ages between 14 and 87 years, who underwent previously scheduled exams. Previously to the determination of absorbed dose by the study sample, dose value measurements were performed in phantoms by means of an ionization chamber, in order to verify whether the obtained values were compliant with those presented by the CT apparatus and whether such values were within the diagnostic reference levels recommended by the European Guidelines(1). Subsequently, the received dose values for abdominal CT were measured, and their relationship with the patients' anthropometric characteristics was studied. Finally, the doses to organs were simulated by means of the Monte Carlo method with the CT-Expo V 1.5 software, and the effect of the automatic exposure control in such examinations was studied. The results were analyzed with the SPSS V16.0 software. Verification of the CT apparatus dose value The CTDIs of the CT apparatus were evaluated by means of dose measurements in acrylic phantoms, with an ionization chamber and an electrometer(8). The dose values were measured with the routine scan protocol for skull, chest, upper abdomen and pelvis. For the measurement of the dose In order to measure the dose in the skull scan, a head phantom with 16 cm in diameter and 15 cm in height was utilized, while for the chest, abdomen and pelvis scans a body phantom with 32 cm in diameter and 15 cm in height was utilized. The value corresponding to CTDI100 was measured at the center of each phantom and at four different peripheral points, and from those values the weighted average was calculated [CTDIW (equation 1)](7).  Finally, the CTDIVol was obtained, taking into consideration the pitch utilized in the images acquisition (equation 2)(7).  The DLP value was calculated by multiplying the CTDIVol by the length of the acquisition L (equation 3)(7).  The effective dose (E) was calculated by multiplying the DLP value by a specific conversion factor for each region, EDLP (equation 4)(7). Measurement of anthropometric characteristics of the patients The data related to the patients comprising the study sample were obtained by utilizing a bioelectrical impedance scale and measurement tapes: body mass, fat mass, lean mass, total body water, height, BMI and abdominal perimeter (at the level of the iliac crests). The patients were duly approached with full explanation of the type of measurements to be performed and by requesting their consents for such. Considering that the BMI corresponds to the body mass in relation to individual differences in height, it is an effective tool for identifying obesity, allowing for its classification into subgroups, as follows(9): insufficient weight (< 18.5 kg/m2); normal weight (18.624.9 kg/m2); excessive weight (25.029.9 kg/m2); class I obesity (30.034.9 kg/m2); class II obesity (35.039.9 kg/m2); and class III obesity (> 40.0 kg/m2). Determination of dose at abdominal CT scans In the present study, the scans were performed in a Siemens Somatom Emotion 6 apparatus, a spiral multislice system (6 slices). For abdominal CT, two protocols were utilized, as follows: a) for a part of the sample (80 patients), a routine protocol of the service was utilized, with 130 kVp, reference of 100 mAs, 6 × 2.0 mm collimation, 1.25 pitch, rotation time of 0.6 s; b) for the remaining 20 patients, an earlier protocol was utilized, with 120 mAs reference and 0.85 pitch, with the other parameters unchanged. The utilization of such two protocols allowed a comparison of the dose values. Some of the patients also underwent pelvic CT scans, besides the abdominal CT. The parameters from such pelvic CT scans were utilized to supplement the present study and to compare the dose values. Most of the scans comprised two series, a non-contrast-enhanced (pre-contrast) and a contras-enhanced (post-contrast) series, depending on the clinical indications. Determination of organ dose The dose to organs was calculated only for those patients who underwent both abdominal and pelvic CT, by means of the simulation software CT-Expo V 1.5, based on the Monte Carlo method. All dose calculations were performed on mathematical phantoms where the male sex is represented by a 1.70 m tall and 70 kg phantom, while the female sex is represented by 1.60 m tall and 60 kg phantom(10). The following acquisition parameters were introduced in the calculations: kVp, mAs, feed/rotation, collimation, beginning and end of the acquisition. Effect of the automatic exposure control The CT apparatus utilized in the present study was equipped with an automatic exposure control application, the CARE Dose 4D, which allows the tube current modulation according to the patient dimensions, thus obtaining a balance between image quality and low radiation dose levels, i.e., allowing to reduce or increase the effective mAs values, depending upon the patient dimensions(11,12). RESULTS The main results obtained in the present study are described in the following paragraphs. Firstly, the results regarding the dose values measured by the CT apparatus are presented, followed by the results regarding the anthropometric characteristics of the patients, the CT scans dose values and the relationship between effective dose and anthropometric characteristics of the patients. Finally, the results regarding organ doses are demonstrated, as well as the effect of the automatic exposure control. Verification of the CT apparatus dose values The dose values obtained with the ionization chamber and those obtained from the CT Siemens Somatom Emotion 6 apparatus on phantoms are presented on Table 1 for routine skull, chest abdomen and pelvis scans. The reference dose values recommended by the European Guidelines are presented on Table 2. 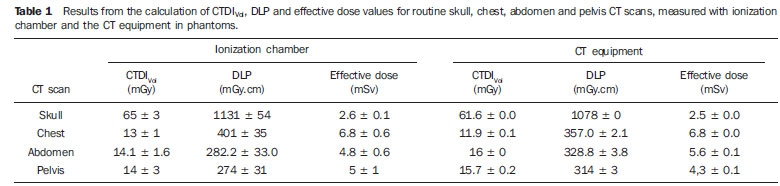 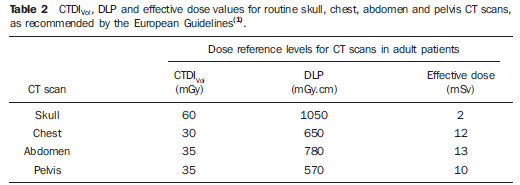 Anthropometric characteristics of the patients The ages of the patients included in the study sample ranged between 14 and 87 years, and 44 of them were women and 56, men. The patients' body mass ranged between 39.2 and 104.2 kg, and height ranged between 1.40 m and 1.82 m, with the BMI ranging between 15.9 and 45.4 kg.m2. The mean values for anthropometric parameters of the sample are the following: 59.5 years of age, height of 1.55 m, 63.63 kg of body mass, 21.99 kg of fat mass, 41.64 kg of lean mass, 30.49 kg of total body water, 93 cm of abdominal perimeter and BMI of 26.51 kg.m2. Abdominal CT scan dose All the patients in the sample underwent abdominal CT; among tem 41 underwent only non-contrast-enhanced CT, while the remaining patients underwent both noncontrast-enhanced and contrast-enhanced CT. Additionally to the abdominal scan, 63 patients also underwent pelvic CT scans. Out of such patients, 29 underwent noncontrast-enhanced CT, 14 underwent only contrast-enhanced CT, and 20 patients underwent both the techniques. The main clinical indication for such examinations was the presence of a tumor (75%), particularly colon carcinomas (17%) and lung neoplasms (12%). Thus the main organs of interest for diagnosis at abdominal scans were the liver and adrenal glands for investigation of metastases, while the main organ of interest at the pelvic scans was the colon, once carcinoma in such an organ is the main clinical indication. As regards radiation dose received by patients during the abdominal and pelvic CT scans performed under the different protocols, the mean values for CTDIVol, DLP and effective dose are presented on Table 3. The values for CTDIVol and DLP were retrieved from the CT equipment protocols and the effective dose was calculated by means of equation 4. 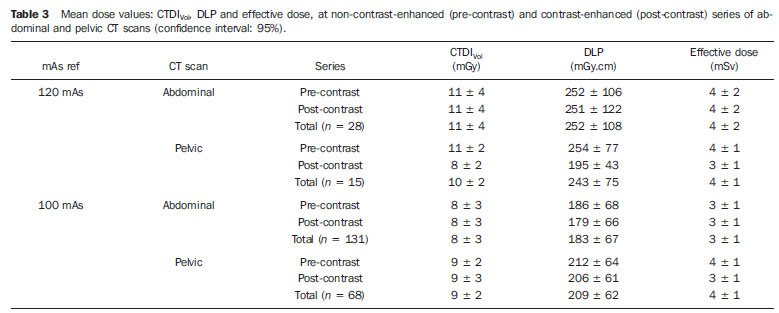 Relationship between effective dose and anthropometric characteristics With the purpose of establishing the relationship between effective dose values (calculated according to equation 4) and patients' anthropometric characteristics, statistical tests of correlation and linear regression were undertaken. Thus, the effective dose was analyzed as a function of sex, age, height, abdominal perimeter, body mass, fat mass, lean mass, total body water and BMI. In the analysis as a function of sex, one observed that male patients received a higher dose during abdominal CT scans and a lower dose during pelvic CT scans, in relation to female patients. As regards age and height, no influence was observed on the effective received dose. As regards patients' abdominal perimeter, one observed that such factor does influence the received dose, with the same being true with body composition, i.e., the effective dose increases as body mass, fat mass, lean mass, total body water and BMI increase. Figure 1 graphically represents the effective received dose at abdominal and pelvic CT scans as a function of abdominal perimeter, body mass and BMI. Such parameters are those which most influenced the effective dose, having been grouped in intervals in order to avoid some results dispersion. The mean effective dose is presented for every such intervals. 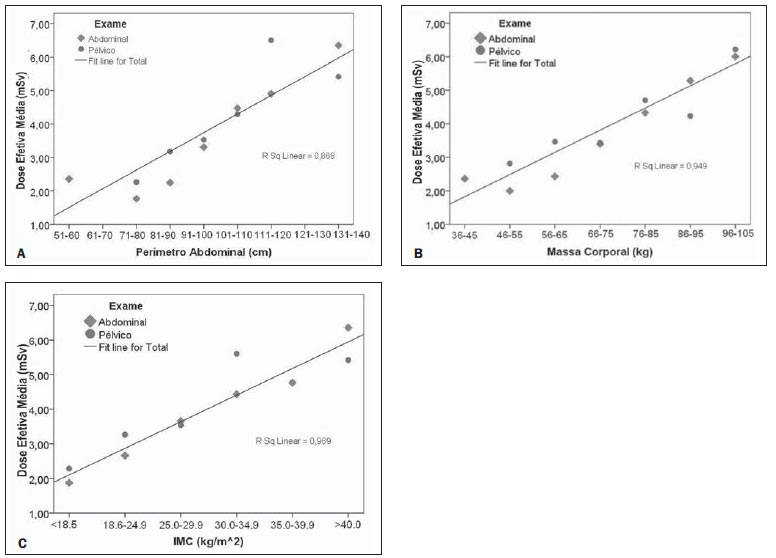 Figure 1A. Graphic representation of mean effective dose as a function of abdominal perimeter, and respective linear regression at abdominal and pelvic CT scans. Figure 1B. Graphic representation of mean effective dose as a function of body mass, and respective linear regression at abdominal and pelvic CT scans. Figure 1C. Graphic representation of mean effective dose as a function of BMI, and respective linear regression at abdominal and pelvic CT scans. The linear regression (R2) results between effective dose and abdominal perimeter, body mass and BMI were 0.868, 0.949 and 0.969, respectively, while the correlation (Pearson's R) between the effective dose and such same parameters were 0.694, 0.754 and 0.695 respectively, for p < 0.01. Dose to organs As previously mentioned, the mean dose to organs was calculated for each type of scan based on the Monte Carlo method and is represented on the chart on Figure 2. 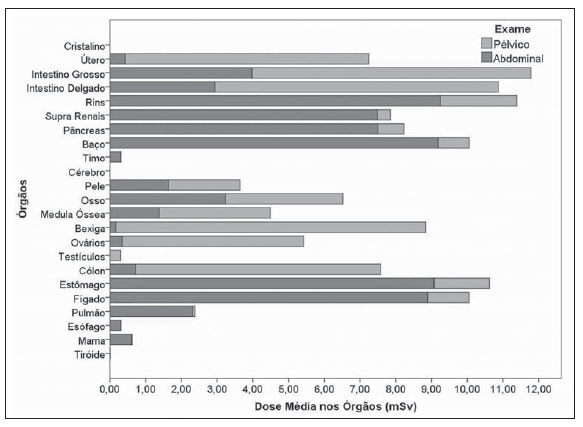 Figure 2. Mean dose to the organs for abdominal and pelvic CT scans, calculated by means of the CT-Expo V 1.5 software. In total, the organs receiving higher radiation doses are the large bowel, the small bowel, the kidneys, the adrenal glands, the pancreas, the spleen, the stomach and the liver. At pelvic scans, the organs receiving higher radiation doses are the uterus, the small bowel, the bladder, the ovaries and the colon. Effect of the automatic exposure control In the evaluation of the automatic exposure control, only the CT scans performed with the reference 100 mAs were analyzed. The utilization of the equipment's software CARE Dose 4D, allowed the adjustment of mAs for the scans, considering the contrast-enhanced and non-contrast-enhanced series, reducing such value in 173 of such series, while increasing it in 22 series and keeping it unchanged in only 4 series. At the abdominal CT scans, where the mAs reduction occurred, the effective mAs values ranged between 37.0 and 97.0 mAs, while at the pelvic CT scans, under the same conditions, the effective mAs values ranged between 48.0 and 96.0 mAs. The mean mAs reduction at the abdominal CT scans was 35.34%, and at the pelvic scans, the mean reduction was 31.03%. Figure 3 presents the charts of mAs values as a function of patient's BMI, at abdominal and pelvic CT scans. 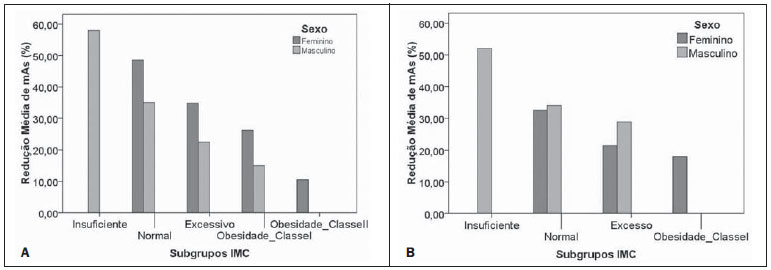 Figure 3. Graphic representation of mean mAs reduction as a function of BMI subgroup at abdominal (A) and pelvic (B) CT scans performed at the 100 mAs reference, for both male and female patients. As previously mentioned, the CARE Dose 4D software also allows to increase the mAs value in the case of patients with higher BMIs, in such a way to maintain a good diagnostic quality of the images. At the abdominal CT scans, the mAs values ranged between 104.0 and 146.0 mAs, while at the pelvic CT scans the values ranged between 107.0 and 148.0 mAs. The mean increase in mAs value at the abdominal scans was 22.8%, while at the pelvic scans it was 20.1%. DISCUSSION Verification of the CT apparatus dose values The results obtained for the CT equipment dose values measured by means of the ionization chamber on the head and body phantoms, demonstrated that the Siemens Somatom Emotion 6 apparatus utilized in the present study was calibrated according to the dose conditions applied in the routine protocols for skull, chest, abdomen and pelvis. The results have also demonstrated that the dose values at such CT scans did not exceed the diagnostic reference levels recommended by the European Guidelines(1). Abdominal CT scan dose Most of the patients underwent both contrast-enhanced and non-contrast-enhanced CT scans (59 patients), and 63 also underwent pelvic CT scans, of which 20 patients were submitted to both series. Based on the dose results obtained at such scans, it was observed that a patient who underwent both abdominal and pelvic CT scans, both with two series, received a total effective dose of 13.29 mSv. As previously mentioned, such dose value represents some risk for induction of cancer, as a dose of 10 mSv has a 1/1,000 probability of cancer induction(6). In the present study, two different protocols were utilized, one with 120 mAs and the other with 100 mAs. In the first case the mean effective dose was 4.28 mSv at the abdominal CT scan, and 4.12 mSv at the pelvic CT scan, while in the second case the mean effective dose was 3.12 mSv at the abdominal CT scan, and 3.55 mSv at the pelvic CT scan. With both protocols, the dose values are lower than the diagnostic reference levels (13.25 mSv for abdomen and 9.69 mSv for the pelvis). As expected, the lower the current × time (mAs) product is, the lower is the dose(7). At the pelvic CT scans, the mean dose was higher than that at abdominal CT scans. Such difference is due to the presence of structures with different densities in those regions. The pelvic region is constituted by more bone structures than the abdominal region. Another o fact was that, at contrast-enhanced scans, the mean effective dose was lower as compared with the non-contrastenhanced scans. Such a fact is explained by a more restricted range adjustment (acquisition area) to the region of interest. In a study developed in Malaysia on abdominal CT scan doses, the effective dose values were higher (7.2 mSv) than those obtained in the present study(13). Such a difference is essentially due to the equipment and acquisition protocols being different. Relationship between effective dose and anthropometric characteristics In the evaluation of the relationship between the effective dose and the patients' anthropometric characteristics, the results demonstrated that the characteristic with greater relationship with effective dose is the body mass, with a high positive linear correlation (R = 0.754 with p < 0.01). Body mass index (R = 0.695), abdominal perimeter (R = 0.694), fat mass (R = 0.634), total body water (R = 0.502), lean mass (R = 0.482) and the percentage of fat mass (R = 0.399), in decreasing order, presented a moderate positive linear correlation (p < 0.01). As regards age and height, such characteristics did not present any statistical significance in the correlation with the effective dose. The results for effective dose as a function of sex demonstrate that at the abdominal CT scans, men receive higher doses, while at the pelvic CT scans, women receive the higher doses. Such a fact is due to differences in anatomical shape, as while men present a larger abdominal perimeter than women, women have a higher pelvic perimeter than men. In another study on the influence of patients' dimensions on the radiation dose, a positive linear correlation was equally obtained between patient's body mass and tube current, i.e., with the effective dose(7,13). Dose to organs As regards the results for dose to organs, it was observed that the organs receiving the higher doses are small bowel, large bowel, uterus, kidneys, adrenal glands, pancreas, spleen, bladder, ovaries, colon, stomach and liver, since they are the main organs positioned in the region of interest and the most radiosensitive ones. Toossi & Dastgherdi have studied the dose to organs at CT scans performed in Iran by means of the CT-Dose software, and concluded that the organs which received higher doses were the same as in the present study(14). Effect of the automatic exposure control In the present study, all the scans were performed with the automatic exposure control, utilizing the CARE Dose 4D application of the CT equipment. Such method allowed the reduction of the radiation dose by means of the decrease of mAs value. The maximum reduction of the mAs value was 63.0% at the abdominal CT scans and 52% at the pelvic scans. The mAs reduction represents a reduction of the equivalent dose, as the dose linearly varies with mAs when all other acquisition parameters are maintained at constant values. Notwithstanding such dose reduction, the application also allowed the increase in mAs values in the cases of patients with higher BMI, so as to maintain the good diagnostic quality of the images, consequently increasing the dose to such patients. In a study developed by Tack et al., it was observed that the reduction in effective mAs was of 15% to 20%, and that such reduction was significantly lower in men than in women, with such a difference being associated to BMI(15). Recommendations for dose optimization The present study has allowed the investigation of the several factors which influence the effective dose received by patients who undergo CT scans, making it possible to develop a set of recommendations in order to optimize the dose in such cases, as follows: 1) Detectors sensitivity Upon the acquisition of CT equipment, it is important to raise questions on the performance of the system and on dose reduction. The apparatuses from different manufacturers are not similar in what concerns detector sensitivity and performance. 2) Maintenance and equipment quality control The repetition of a scan due to equipment failure increases the dose without any benefit to the patient. The implementation of a quality control program allows the minimization of such type of incident. 3) Justification for the scans The risk/benefit factor should be carefully studied, as well as the possibility of resorting to other imaging methods which does not rely on ionizing radiation. 4) Diagnostic reference levels Such levels must be considered so as not to be exceeded during CT scans. 5) Limit the acquisition area to the region of interest a significant dose reduction can be obtained by means of a correct range positioning. 6) Limit the number of series necessary for diagnosis The performance of contrast-enhanced or multi-phase scans of the liver and kidney automatically results in doubling or tripling the dose. 7) Reduce the exposure parameters The dose to patients is directly related to mAs. However, some aspects regarding image quality (contrast resolution, for example) are affected by dose reduction. Thus a proper balance must be found between dose and image quality, where higher noise levels (lower dose) compatible with diagnostic accuracy can be obtained. 8) Adjust the exposure parameters to the patient's dimensions The utilization of automatic exposure control applications is a way to reduce the dose according to the patient's dimensions. In children, pediatric protocols should be utilized, with the exposure parameters adjusted to reduce the dose to such patients according to their ages. 9) Adjust the acquisition parameters to the type of scan In follow-up CT scans, it is possible to reduce the dose, as the main objective of such scans is to monitor the progression of a known lesion. It is important to highlight that in such cases, the number of series to be performed can be reduced, for example, by performing the noncontrast-enhanced scan only for the liver. 10) Training and investigation Review of the protocols utilized in the institution and comparison of image quality and dose with the ICRP recommendations. Training on dose reduction techniques is of utmost importance. The present study should by supplemented by further investigations with a larger sample, since time scarcity was a limiting factor faced by the authors. A study comprising other CT equipment models may also be developed, allowing a comparison of data obtained with different apparatuses. The CT-Expo software also allows dose simulations in other apparatuses, as well as the utilization of other acquisition parameters, allowing comparison between results. CONCLUSION The results obtained in the present study lead to the conclusion that the received radiation dose during abdominal CT scans depend upon some of the patients' characteristics, making it important to adjust the acquisition parameters to the patient's dimensions. An effective method is the utilization of the automatic exposure control, which allows decreasing or increasing tube current according to the patient's dimensions. However, in the case of children, such method alone is not enough. Because of such patients' greater radiosensitivity, special attention should be placed on the utilization of pediatric protocols and in taking all necessary precautions, as well as on complying with all the principles of radiological protection. In some types of CT scans it is possible to perform the image acquisition with a lower dose to the patients. However, that leads to an increase in image noise. Such increased noise is acceptable, provided the images are sufficient to allow an efficient clinical diagnosis (ALARA principle As Low As Reasonably Achievable). Acknowledgements The authors wish to thank the Radiology Department of Hospital de Faro, EPE, Dr. Maria Helena Gomes, the radiology technician Vítor Ferreira, Professors Conceição Abreu and Maria Palma and Engineer João Pires, for the valuable assistance. REFERENCES 1. International Commission on Radiological Protection. Managing patient dose in computed tomography. ICRP Publication 87. Ann ICRP. 2000;30(4). 2. Paterson A, Frush DP. Dose reduction in paediatric MDCT: general principles. Clin Radiol. 2007;62:50717. 3. Silva MSR, Khoury HJ, Borrás C, et al. Dosimetria de pacientes e médicos em intervenções coronárias percutâneas em Recife, Pernambuco, Brasil. Radiol Bras. 2011;44:906. 4. Dalmazo J, Elias Jr J, Brocchi MAC, et al. Otimização da dose em exames de rotina em tomografia computadorizada: estudo de viabilidade em um hospital universitário. Radiol Bras. 2010;43:2418. 5. European Medical ALARA Network. Optimisation of Patient Exposure in CT Procedures. WG1 - SynthDoc - revised3-2011. 6. The National Academies Press. Health risks from exposure to low levels of ionization radiation: BEIR VII phase 2 (2006). [cited 2010 May 15]. Available from: http://www.nap.edu/openbook.php?isbn=030909156X 7. McNitt-Gray MF. AAPM/RSNA physics tutorial for residents: topics in CT. Radiation dose in CT. Radiographics. 2002;22:154153. 8. Rothenberg LN, Pentlow KS. AAPM Tutorial. Radiation dose in CT. Radiographics. 1992;12:122543. 9. World Health Organization. Global database on body mass index. BMI classification. 2008. [cited 2010 July 12]. Available from: http://www.who.int/bmi/index.jsp?introPage=intro_3.html 10. Stamm G, Nagel HD. User's guide CT-Expo V 1.5. A tool for dose evaluation in computed tomography. Hannover-Hamburg; 2005. 11. Imhof H, Schibany N, Ba-Ssalamah A, et al. Spiral CT and radiation dose. Eur J Radiol. 2003;47:2937. 12. Aldrich JE, Chang SD, Bilawich AM, et al. Radiation dose in abdominal computed tomography: the role of patient size and the selection of tube current. Can Assoc Radiol J. 2006;57:1528. 13. Ali MH. Trends in CT abdominal doses in Malaysian practices [tese de doutoramento]. Sidney: Faculty of Health Sciences, University of Sydney; 2005. 14. Toossi MT, Dastgherdi SM. An assessment of organ and effective dose of patients who undertake CT examinations in two teaching hospitals of Mashhad&Isfahan. 11th International Congress of International Radiation Protection Association; 2004 May 23-28; Madrid, Spain. 15. Tack D, De Maertelaer V, Gevenois PA. Dose reduction in multidetector CT using attenuationbased online tube current modulation. AJR Am J Roentgenol. 2003;181:3314. 1. Master, Radiology Technician at Hospital de Faro, EPE, Professor, Department of Radiology, School of Health University of Algarve, Portugal. 2. Master, Fellow PhD degree in Sociology, Member of Research Center CESNOVA Nova Lisbon University, Professor, Department of Radiology, School of Health University of Algarve, Portugal. 3. PhD, Member of Research Center CIDAF University of Coimbra, Professor, Department of Radiology, School of Health University of Algarve, Portugal. 4. Licenciate, Fellow PhD degree of Biomedicine at University of Beira Interior, Professor, Department of Radiology, School of Health University of Algarve, Portugal. Mailing Address: Prof. Rui Almeida Avenida Doutor Adelino da Palma Carlos 8000-510 Faro, Portugal Received June 11, 2012. Accepted after revision September 11, 2012. * Study developed at School of Health University of Algarve, Portugal. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554