Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 5 - Sep. / Oct. of 2012
Vol. 45 nº 5 - Sep. / Oct. of 2012
|
REVIEW ARTICLES
|
|
Bone attrition: a cause of knee pain in osteoarthritis* |
|
|
Autho(rs): Wilson Campos Tavares Júnior1; Fernando Meira de Faria1; Reginaldo Figueiredo2; João Paulo Kawaoka Matushita3; Luciana Costa Silva4; Adriana Maria Kakehasi5 |
|
|
Keywords: Magnetic resonance imaging; Osteoarthritis; Knee pain; Bone attrition; Subchondral bone; Diagnosis. |
|
|
Abstract: INTRODUCTION
Osteoarthritis is a common cause of medical consultations(1). A more comprehensive understanding of osteoarthritis, not only regarding symptoms but also regarding potentially modifiable risks, could lead to the adoption of new strategies in the management of this disease(2). Several factors, including biomechanics, genetics and inflammation determine the heterogeneous nature of osteoarthritis(3). A combination of these factors contributes to the onset of symptoms such as pain, rigidity and joint dysfunction. In this context, knee pain has shown to be the most frequent symptom of osteoarthritis, a condition that is the main cause of chronic disability in the elderly and a big source of deficiency attributable to this condition. The severity of this pain is widely variable, implying from absence of symptoms to immobilization and/or disability of the patient(4). There is little chance that the severity of knee pain in individuals with osteoarthritis constitutes an easily explainable phenomenon. The anatomic fundamentals and the molecular pathogenesis of this condition has been centered on the concept that the onset and progression of the disease are related to the thinning and softening of the joint cartilage, with progressive deterioration of the joint(5). For a long time, the investigations on the structural cause of pain have been focused on cartilaginous defects, even knowing that the cartilage does not contain pain-sensitive fibers(6). Several studies have reported variable associations between knee pain and loss of hyaline cartilage of the joint(7,8). Although osteoarthritis has been traditionally considered as a primary disease of the articular cartilage, emphasis has nowadays been put on the concept that this is a very simplistic conclusion(9), since it is a process which involves articular tissues and structures such as subchondral bone, fibrocartilages, ligaments, muscles, joint capsule and synovial membrane(10). As one can observe in several publications, the sources of pain in osteoarthritis still remain obscure, and the pain may come from any of the different innervated tissues. It is important to highlight that association with other abnormalities such as joint effusion, synovitis and meniscal lesions may be observed. Additionally, subchondral bone may also play a significant role in the generation of pain(11). Currently, emphasis has been given to research involving the causes of knee pain on the grounds of objective findings in the field of imaging diagnosis, particularly, magnetic resonance imaging (MRI)(12,13). In the investigation of knee pain, it is equally important to correlate patients' clinical data and age with possible diseases which are more prevalent in that subgroup. Spontaneous knee osteonecrosis, for example, develops with sudden onset of localized pain, with prevalence in female individuals, notably from the seventh decade of life on, with no association with systemic disorders, alcohol abuse, previous corticosteroid therapy, meniscal surgery or local trauma(14). In younger women, the occurrence of osteonecrosis corroborates the suspicion of any rheumathological disease, particularly systemic lupus erythematosus. In such patients, osteonecrosis causes pain prior to articular destruction(15). Kornaat et al.(8) have evaluated the association of clinical findings and structural abnormalities observed at MRI in patients with osteoarthritis of the knee. The presence of a moderate to large amount of articular fluid could be found in association with knee pain and rigidity. Concomitantly, the presence of osteophytes in the patellofemoral compartment and/or more than four osteophytes in the whole knee were also associated with pain. On the other hand, focal or diffuse cartilaginous abnormalities, subchondral cysts, bone marrow edema, subluxation and/or meniscal lesions or Baker cysts were not associated with pain and rigidity. In summary, the identification of structures actually associated with pain in osteoarthritis of the knee shall contribute to a deeper understanding of this disease and, in the long term, shall allow the adoption of rational therapeutic approaches to this condition. OSTEOARTHRITIS GENESIS In almost of all cases, the joint cartilage is the tissue which presents the major alterations found in cases of osteoarthritis which can be observed both in the primary and secondary presentations of the disease. Among its morphological alterations, one observes that the cartilage loses its homogeneous nature, becoming torn, fragmented, with fibrillation, clefts and ulcerations. Many times, with the progression of the pathological process, the cartilage cannot be seen and, as a consequence, exposed areas of subchondral bone are observed(16). One of the most frequent etiologies in osteoarthritis is the increase in rigidity of the subchondral bone plate, a fact that could trigger cartilage damage involving particularly fibrillation and clefts. The integrity of this tissue is necessary for the normal functioning of the joint(17). In spite of the radiographic subchondral sclerosis being considered as secondary to cartilage damage, a series of reports have been published, suggesting that there may be a fundamental change in such a concept and, therefore, bone sclerosis would really lead to cartilage damage, and not vice-versa(17). Another very interesting information is related to the spongy bone which may be detected adjacent to synovial joints with the important function of cushioning the forces transmitted to the joints. Such forces may be critical in the production of damages to the cartilage in the setting of osteoarthritis, particularly in case of excessive load on the bone(18). In experimental models of osteoarthritis, subchondral bone changes occur precociously after disease induction, revealing noticeable bone remodeling caused by the disease. Such changes occur about two weeks after surgical procedures involving crossed ligaments and in cases of meniscectomy, even before the onset of chondral lesions. In the early stages of the disease, focal damages are observed in the cartilage surface of the medial compartment, and it is import to note that, in this phase, the cartilage thinning process is detected only by histomorphometry(19). Radin et al.(20,21) have described increase in subchondral bone development and decrease in porosity in an animal model of osteoarthritis, in association with a relative rigidity of the bone. After a precocious bone change, the occurrence of deep fibrillation of the superjacent joint cartilage. WHAT IS BONE ATTRITION? Everything indicates that bone attrition might represent subchondral bone remodeling in cases of osteoarthritis and, as a result, promote changes in the shape and contours of the bone, or even cause bone tissue loss(22). Bone attrition is the least studied alteration of the subchondral bone, and is evaluated at conventional radiography as loss of bone density(23) or, at MRI, as flattening/depression of the articular cortex(24). The presence of bone attrition was strongly associated with cartilage loss along time, occurring in the bone tissue located in the same region of cartilage loss in the knee(25). Such findings were consistent in both compartments of the knee, in spite of suggesting that the most noticeable effects were observed in specific areas which supported higher load. It is important to highlight that the cartilage and underlying bone may undergo changes in osteoarthritis, as a result from the load transmitted to such tissues. Bone attrition influences the loss of the overlying cartilage as a result from changes in the bone surface, so this structure becomes more vulnerable to the load. Therefore, such attrition may serve as a marker for an area submitted to compressive forces where cartilage loss becomes inevitable(18,25). In recent studies approaching the osteoarthritis etiopathogenesis, Lories(26) and Brandt et al.(27) have concluded that, currently, it is commonly accepted that, after an initial aggression, complex interactions between several mechanisms of bone repair and regeneration may explain many of the late joint alterations observed in the disease. CAUSES OF BONE ATTRITION Knee misalignment may be associated with an increase in prevalence and incidence of subchondral bone attrition in a specific compartmental presentation(28). For example, in cases of varus deformity of knee, the mechanical stress is transmitted by the medial compartment. Such deformity is related with increased risk for progression of the structural damages visualized in knees with pre-existing osteoarthritis and with the loss of cartilage in the involved compartment. Additionally, a multicentric study about osteoarthritis (MOST) has shown that knee misalignment was associated with bone attrition in the compartment submitted to greater stress(18,25,27,29-32). Attrition may represent alterations in bone remodeling as a response to mechanical forces acting on the bone(33). The contribution of bone marrow lesions to the pain severity depends on the presence of subarticular bone attrition(34). Such lesions are considered as a reflection of the misalignment in the specific joint compartment(35,36). Joint stress leads to subchondral bone remodeling, with consequential attrition in these areas undergoing greater stress(37). CLINICAL MANIFESTATIONS OF BONE ATTRITION In a cross sectional study, Neogi et al.(25) have suggested that bone attrition is associated with knee pain, and such an association was most noticeable in knees where osteoarthritis could not be visualized at conventional radiography, suggesting that bone attrition participates in the genesis of pain at early or intermediate stages of the disease. Dieppe et al.(23) have reported evidences of a possible relation between radiographically observed bone attrition and night pain. In another study utilizing MRI and involving 143 individuals with painful osteoarthritis of knee, Dieppe(38), reported that the pain intensity was associated with bone attrition, bone marrow lesion, meniscal lesions and synovitis/effusion. In cases where bone attrition is detected at conventional radiography, the probability of the patient presenting pain, rigidity and physical disability increases in twothree times. As radiographic bone images are interpreted, attention should be paid not only to the reduction of joint space and osteophytes, but also to the subchondral bone(39). Change in the bone contours and surface could result from subchondral bone remodeling, including fibrosis, necrosis and focal collapse of the bone, being ultimately responsible for the joint pain(40-42). DIAGNOSIS AND CLASSIFICATION Bone attrition is not easily recognizable. It may be hardly detected in the absence of clear defects of the cortical bone integrity and because of overlap of bone structures at plain radiography. In 1968, Ahlbäck(43) introduced a classification system including an evaluation of bone attrition by means of conventional radiography. Considering the subtleness of alterations at conventional radiography and, in the absence of cortical bone abnormalities, the appearance of such alterations is almost the same either at MRI or computed tomography (CT). However, the latter two methods present the advantage of allowing multiplanar visualization. At conventional radiography, MRI and CT, bone attrition is interpreted as flattening or depression of articular surfaces, and classified with basis on a subjective degree of deviation from the normal contour on different images, as follows: grade 0 = normal; grade 1 = moderate; grade 3 = severe (Figure 1)(24). 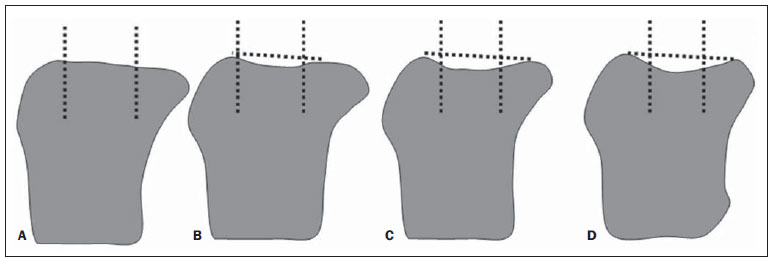 Figure 1. Grade 0 (normal) (A), grade 1 (mild) (B), grade 2 (moderate) (C), grade 3 (severe) (D). Classification of subarticular bone attrition based on the degree of articular surface flattening or depression as compared with normality. Modified from Peterfy et al.(24). For example, the articular surfaces of the femoral condyles and of the medial aspect of the patella are generally slightly convex. Thus, the normal convexity is shown on Figure 2, while flattening of such structures corresponds to grade 1 (Figure 3), mild concavity corresponds to grade 2 (Figure 4) and severe concavity, to grade 3 (Figure 5).  Figure 2. Grade 0 (normal). Sagittal MRI of knee, T2-weighted image with fat saturation, with no sign of structural alterations. 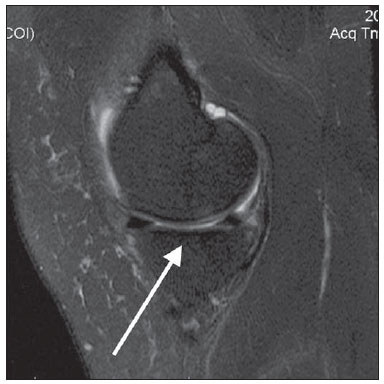 Figure 3. Grade 1 (mild). Sagittal MRI of knee, T2-weighted image with fat saturation. Signs of subtle infradeleveling of the tibial plateau, suggesting bone attrition observed on the medial tibial plateau. 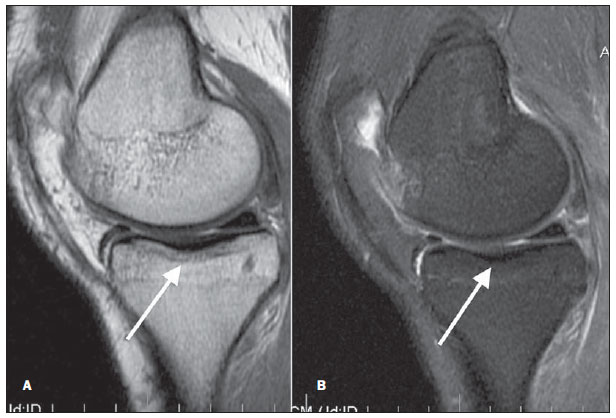 Figure 4. Grade 2 (moderate). Sagittal MRI of the knee, T1- (A) and T2-weighted (B) images with fat suppression. Moderate infradeleveling of the tibial plateau, also with signs of subtle subchondral sclerosis characterized by hyposignal intensity on the T1-weighted image, suggesting the presence of bone attrition on the medial tibial plateau. 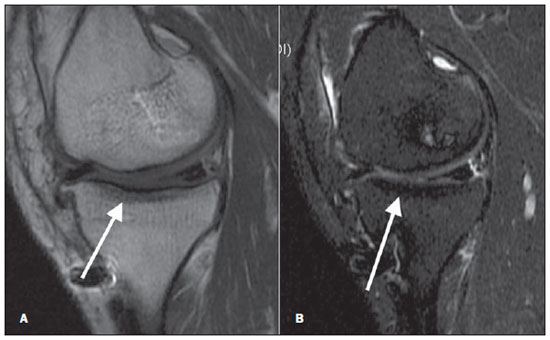 Figure 5. Grade 3 (severe). Sagittal MRI of the knee, T1- (A) and T2-weighted (B) images with fat suppression. Signs of marked infradeleveling of the tibial plateau and moderate loss of concavity with rectification of the femoral condyle, in association with signs of subchondral sclerosis in the tibial plateau, suggesting bone attrition observed on the medial tibial plateau and on the femoral condyle. Signs of involvement of the hyaline cartilage represented by changes in signal intensity and thinning. MRI has shown to be superior to plain radiography because it can demonstrate the knee joint in conjunction with its internal structures(42). CT has been less utilized, since it lacks clearness in demonstrating some knee internal structures such as the meniscus and cartilage. On the other hand, MRI can clearly demonstrate all the internal structures of the knee as well as bone remodeling and eventual signal alterations(44). Occurrence of bone attrition before advanced osteoarthritis could suggest that bone changes occur simultaneously with cartilage loss and that treatments aimed at cartilage recovery will not be effective, even in cases where the disease is not advanced yet. MRI studies suggest that many knees with radiographically moderate osteoarthritis, without narrowing of the articular space, present some evidence of bone attrition(45). DISCUSSION Articular pain may become a limiting factor and even a cause of disability in the patient's life, and may affect any joint in the human body(46,47). The literature presents discordant information on the actual causes of pain in osteoarthritis patients, but recent multicentric studies, such as MOST(28,30), have demonstrated the association between bone attrition and pain. Findings related to bone attrition have ever been present at conventional radiography, but, maybe because of the difficulty in defining such findings by means of this method, it was not very diffused in the routine clinical assessment(48). Currently, with the availability of high resolution sectional imaging methods and high-field MRI apparatuses, such alterations can be clearly defined, allowing the adoption of an approach to pain in patients with bone attrition. It is important to highlight that, up to the present moment, the literature does not report a specific treatment for pain related to bone attrition. With the technological progress, a new research field is emerging for treatment and follow-up of these patients. CONCLUSIONS Further studies could offer a deeper understanding of the true bone attrition thresholds, preferentially encompassing an independent reading of bone attrition and other characteristics of osteoarthritis. Cartilage loss is seen as a remarkable characteristic in the development of osteoarthritis and, up to the present moment, the bone response becomes noticeable only at late stages of the process. Thus, the evaluation of the chondral bone may become important in future researches related to the mechanisms of pain generation and also for development of new therapeutic strategies. The involvement of the subchondral bone at early stages of the disease may help to explain the failure of chondroprotective agents just like that occurring with disease-modifying drugs. Studies with sodium MRI and with a field higher than the current 1.5T standard could be utilized to investigate relevant data involving the bone attrition biochemistry and physiology. Finally, the prevalence of bone attrition in cases of non-advanced osteoarthritis is substantial, and physicians should be aware of the relevance and of the ways of diagnosing and describing such finding on images of these patients of this condition. REFERENCES 1. Cisternas MG, Yelin E, Katz JN, et al. Ambulatory visit utilization in a national, populationbased sample of adults with osteoarthritis. Arthritis Rheum. 2009;61:1694-703. 2. Jüni P, Reichenbach S, Dieppe P. Osteoarthritis: rational approach to treating the individual. Best Pract Res Clin Rheumatol. 2006;20:721-40. 3. Peterfy CG, Gold G, Eckstein F, et al. MRI protocols for whole-organ assessment of the knee in osteoarthritis. Osteoarthritis Cartilage. 2006;14 Suppl A:A95-111. 4. Clauw DJ, Witter J. Pain and rheumatology: thinking outside the joint. Arthritis Rheum. 2009;60:321-4. 5. Hudelmaier M, Glaser C, Hohe J, et al. Age-related changes in the morphology and deformational behavior of knee joint cartilage. Arthritis Rheum. 2001;44:2556-61. 6. Felson DT. The sources of pain in knee osteoarthritis. Curr Opin Rheumatol. 2005;17:624-8. 7. Wluka AE, Wolfe R, Stuckey S, et al. How does tibial cartilage volume relate to symptoms in subjects with knee osteoarthritis? Ann Rheum Dis. 2004;63:264-8. 8. Kornaat PR, Bloem JL, Ceulemans RY, et al. Osteoarthritis of the knee: association between clinical features and MR imaging findings. Radiology. 2006;239:811-7. 9. Brandt KD, Radin EL, Dieppe PA, et al. Yet more evidence that osteoarthritis is not a cartilage disease. Ann Rheum Dis. 2006;65:1261-4. 10. Hunter DJ, Felson DT. Osteoarthritis. BMJ. 2006;332:639-42. 11. Hill CL, Gale DG, Chaisson CE, et al. Knee effusions, popliteal cysts, and synovial thickening: association with knee pain in osteoarthritis. J Rheumatol. 2001;28:1330-7. 12. Torres L, Dunlop DD, Peterfy C, et al. The relationship between tissue lesion and pain severity in persons with knee osteoarthritis. Osteoarthritis Cartilage. 2006;14:1033-40. 13. Hunter DJ, Lo GH, Gale D, et al. The reliability of a new scoring system for knee osteoarthritis MRI and the validity of bone marrow lesion assessment: BLOKS (Boston Leeds Osteoarthritis Knee Score). Ann Rheum Dis. 2008;67:206-11. 14. Cunha DL, Carvalho ACP, Ribeiro EJS, et al. Ressonância magnética da osteonecrose do joelho: estudo de 19 casos. Radiol Bras. 2010;43:77-80. 15. Ribeiro DS, Araújo Neto C, D'Almeida F, et al. Achados de imagem das alterações musculoesqueléticas associadas ao lúpus eritematoso sistêmico. Radiol Bras. 2011;44:52-8. 16. Rezende MU, Hernandez AJ, Camanho GL, et al. Cartilagem articular e osteoartrose. Acta Ortop Bras. 2000;8:100-4. 17. Imhof H, Breitenseher M, Kainberger F, et al. Degenerative joint disease: cartilage or vascular disease? Skeletal Radiol. 1997;26:398-403. 18. Radin EL, Paul IL, Rose RM. Role of mechanical factors in pathogenesis of primary osteoarthritis. Lancet. 1972;1:519-22. 19. Hayami T, Pickarski M, Zhuo Y, et al. Characterization of articular cartilage and subchondral bone changes in the rat anterior cruciate ligament transection and meniscectomized models of osteoarthritis. Bone. 2006;38:234-43. 20. Radin EL, Martin RB, Burr DB, et al. Effects of mechanical loading on the tissues of the rabbit knee. J Orthop Res. 1984;2:221-34. 21. Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of cartilage damage. Clin Orthop Relat Res. 1986;(213):34-40. 22. Burr DB. The importance of subchondral bone in the progression of osteoarthritis. J Rheumatol Suppl. 2004;70:77-80. 23. Dieppe PA, Reichenbach S, Williams S, et al. Assessing bone loss on radiographs of the knee in osteoarthritis: a cross-sectional study. Arthritis Rheum. 2005;52:3536-41. 24. Peterfy CG, Guermazi A, Zaim S, et al. Whole- Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthritis Cartilage. 2004;12:177-90. 25. Neogi T, Felson D, Niu J, et al. Cartilage loss occurs in the same subregions as subchondral bone attrition: a within-knee subregion-matched approach from the Multicenter Osteoarthritis Study. Arthritis Rheum. 2009;61:1539-44. 26. Lories RJ. Joint homeostasis, restoration, and remodeling in osteoarthritis. Best Pract Res Clin Rheumatol. 2008;22:209-20. 27. Brandt KD, Dieppe P, Radin EL. Etiopathogenesis of osteoarthritis. Rheum Dis Clin North Am. 2008;34:531-59. 28. Neogi T, Nevitt M, Niu J, et al. Subchondral bone attrition may be a reflection of compartment-specific mechanical load: the MOST Study. Ann Rheum Dis. 2010;69:841-4. 29. Dieppe P, Cushnaghan J, Young P, et al. Prediction of the progression of joint space narrowing in osteoarthritis of the knee by bone scintigraphy. Ann Rheum Dis. 1993;52:557-63. 30. Roemer FW, Neogi T, Nevitt MC, et al. Subchondral bone marrow lesions are highly associated with, and predict subchondral bone attrition longitudinally: the MOST study. Osteoarthritis Cartilage. 2010;18:47-53. 31. Sharma L, Song J, Felson DT, et al. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA. 2001;286:188-95. 32. Hunter DJ, Zhang Y, Niu J, et al. Structural factors associated with malalignment in knee osteoarthritis: the Boston osteoarthritis knee study. J Rheumatol. 2005;32:2192-9. 33. Hernández-Molina G, Neogi T, Hunter DJ, et al. The association of bone attrition with knee pain and other MRI features of osteoarthritis. Ann Rheum Dis. 2008;67:43-7. 34. Torres L, Dunlop DD, Peterfy C, et al. The relationship between specific tissue lesions and pain severity in persons with knee osteoarthritis. Osteoarthritis Cartilage. 2006;14:1033-40. 35. Felson DT, McLaughlin S, Goggins J, et al. Bone marrow edema and its relation to progression of knee osteoarthritis. Ann Intern Med. 2003;139(5 Pt 1):330-6. 36. Hunter DJ, Zhang Y, Niu J, et al. Increase in bone marrow lesions associated with cartilage loss: a longitudinal magnetic resonance imaging study of knee osteoarthritis. Arthritis Rheum. 2006;54:1529-35. 37. Dequeker J. The relationship between osteoporosis and osteoarthritis. Clin Rheum Dis. 1985;11:271-96. 38. Dieppe P. Subchondral bone should be the main target for the treatment of pain and disease progression in osteoarthritis. Osteoarthritis Cartilage. 1999;7:325-6. 39. Reichenbach S, Dieppe PA, Nüesch E, et al. Association of bone attrition with knee pain, stiffness and disability: a cross-sectional study. Ann Rheum Dis. 2011;70:293-8. 40. Zanetti M, Bruder E, Romero J, et al. Bone marrow edema pattern in osteoarthritic knees: correlation between MR imaging and histologic findings. Radiology. 2000;215:835-40. 41. Martig S, Boisclair J, Konar M, et al. MRI characteristics and histology of bone marrow lesions in dogs with experimentally induced osteoarthritis. Vet Radiol Ultrasound. 2007;48:105-12. 42. Bergman AG, Willén HK, Lindstrand AL, et al. Osteoarthritis of the knee: correlation of subchondral MR signal abnormalities with histopathologic and radiographic features. Skeletal Radiol. 1994;23:445-8. 43. Ahlbäck S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol Diagn (Stockh). 1968;Suppl 277:7-72. 44. Yusuf E, Kortekaas MC, Watt I, et al. Do knee abnormalities visualised on MRI explain knee pain in knee osteoarthritis? A systematic review. Ann Rheum Dis. 2011;70:60-7. 45. Reichenbach S, Guermazi A, Niu J, et al. Prevalence of bone attrition on knee radiographs and MRI in a community-based cohort. Osteoarthritis Cartilage. 2008;16:1005-10. 46. Melo Junior CF, Saito OC, Guimarães Filho HA. Avaliação ultrassonográfica dos distúrbios intracapsulares temporomandibulares. Radiol Bras. 2011;44:355-9. 47. Lima CMAO, Ribeiro EB, Coutinho EPD, et al. Síndrome do impacto do tornozelo na ressonância magnética: ensaio iconográfico. Radiol Bras. 2010;43:53-7. 48. Albuquerque RP, Carvalho ACP, Giordano V, et al. Estudo comparativo entre incidências radiográficas para a osteoartrose do joelho. Acta Reumatol Port. 2009;34:380-7. 1. MDs, Radiologists, Hospital das Clínicas da Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. 2. PhD, Associate Professor, Department of Complementary Diagnostic Work-up, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. 3. PhD, Associate Professor, Department of Complementary Diagnostic Work-up, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. 4. Master, Assistant Professor, Department of Complementary Diagnostic Work-up, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. 5. PhD, Associate Professor, Department of Locomotor System, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. Mailing Address: Dr. Wilson Campos Tavares Júnior Rua Gonçalves Dias, 750/1803, Funcionários Belo Horizonte, MG, Brazil, 30140-091 E-mail: wilsoncamp2000@yahoo.com.br Received April 25, 2012. Accepted after revision August 20, 2012. * Study developed at Hospital das Clínicas da Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554