Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 2 - Mar. / Apr. of 2012
Vol. 45 nº 2 - Mar. / Apr. of 2012
|
CASE REPORT
|
|
Madelung's disease: a case report and literature review |
|
|
Autho(rs): Ligia Persici Rodrigues1; Ernesto Lima Araujo Melo2 |
|
|
Keywords: Madelung's disease; Benign multiple symmetric lipomatosis; Lipomas; Alcoholism. |
|
|
Abstract: INTRODUCTION
Multiple symmetric lipomatosis, also known as Madelung's disease or Launois- Bensaude syndrome, is a rare entity characterized by painless, subcutaneous diffuse deposition of adipose tissue on the neck, upper trunk, arms and legs(1). Historically, Madelung's disease has been most frequently observed in men (male-female ratio = 15:1) aged between 30 and 60 years. The disease prevalence is increased among the Mediterranean population (reported incidence in Italy: 1/25,000 men), and there is a relationship between this disease and excessive consumption of alcohol, particularly red wine(2). Such a condition develops over a period of months to years. The patients complain of their appearance although, in advanced cases, the increase in fat deposits may cause dyspnea or dysphagia(3). Association of Madelung's disease with diabetes, gout, alcoholism and other systemic diseases has been observed(4). The authors report the case of a 50-yearold man with painless masses in the cervicofacial region and in the upper trunk, which increase over a period of three to four years (Figure 1).  Figure 1. Lateral and frontal views of the patient demonstrating symmetrical enlargement of soft tissues resulting from fat deposition. CASE REPORT The patient's clinical history indicated systemic arterial hypertension effectively controlled with medication. The patient denied increase in caloric intake and reported alcohol consumption of 1.0 liter of distilled beverage per day during 28 years. At physical examination, foci of volume increase were observed on the face, neck and upper trunk, with no sign of edema. Subsequently, the patient was submitted to head and neck computed tomography (CT) with basis on a clinical hypothesis of lipomas. The CT findings showed a symmetric and diffuse subcutaneous distribution of homogeneous, nonencapsulated adipose material in the cervicofacial region and the upper trunk, with no sign of contrast enhancement. The deep muscle planes demonstrated preserved morphologies, contours and attenuation coefficients, slightly displaced by the adipose material, but with no signs of direct infiltration. Lymph node enlargement, mass with soft tissue attenuation, marked lymphatic malformations or vascular dilatation were not observed (Figure 2). 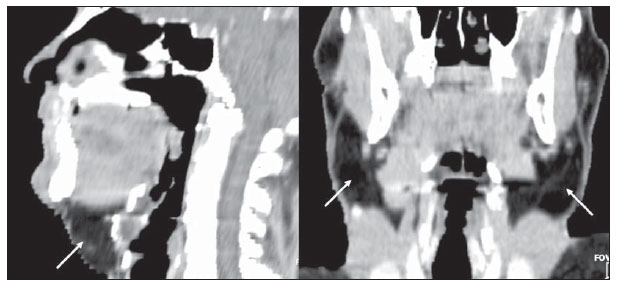 Figure 2. Sagittal and coronal reconstructions demonstrating deep and diffuse deposition of adipose tissue (arrows). DISCUSSION Madelung was the first author to extensively describe this entity in a series of patients in 1888; hence the name Madelung's disease. In 1889, Launois and Bensaude reported 65 cases, expanding the description of this disease that also has been called as Launois-Bensaude syndrome. Currently, reports on more than 270 cases are found in the literature(2,5). Multiple symmetric lipomatosis is classified into two types, as follows: type I, with lipomatous masses in the parotid region, neck, suprascapular and deltoid regions. In this group, deep involvement causing dyspnea and dysphagia may be observed in some patients. In type II, lipomatosis is diffuse, with clinical appearance of simple obesity, and without the symptoms of deep involvement present in type I(6). Typically, the masses do not respect cleavage planes, penetrating all levels of the tissue, so their surgical exeresis is more difficult(4). Several types of lipomatosis typically differentiated by anatomic location and varied clinical symptoms have been described. Such types include multiple symmetric lipomatosis, congenital infiltrative lipomatosis of the face, encephalocraniocutaneous lipomatosis, scapular waist lipomatosis, adiposis dolorosa, pelvic lipomatosis and mediastinal lipomatosis(5). The clinical diagnosis is based on the recognition of the unique appearance of the patient, but in atypical cases, there may be confusion with lymphoproliferative disorders and other conditions(4). The etiology of Madelung's disease still remains unknown. Alcohol ingestion of more than 80 g per day during at least ten years a factor observed in up to 90% of cases described in the literature -, was also observed in the present case. Polyneuropathy, described as a sensory, motor and autonomic dysfunction, and detected in about 85% of patients with Madelung's disease, generally develops several years after the onset of lipomas, and was not present in this case(7). Chest radiography may show mediastinal enlargement. At CT, lipomatous, nonencapsulated and homogeneous tissue is observed, possibly in association with deep deposition (submuscular) of adipose tissue (Figure 3). This latter presentation is most frequently observed around the trachea and/or deeply located in the trapezius muscle. In some cases, calcifications are identified within lipomas(7). 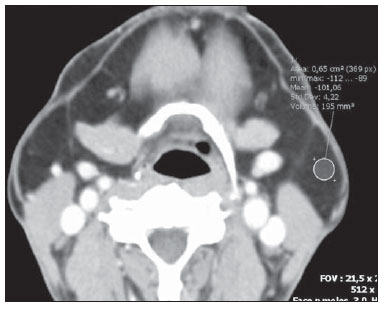 Figure 3. Contrast-enhanced axial image demonstrating diffuse deposition of adipose tissue involving deep structures. Currently, CT is considered to be the method of choice for the diagnosis, preoperative staging and postoperative follow-up of patients with multiple symmetric lipomatosis. The evaluation of images directly on the CT display screen, on workstations or on computers equipped with visualization software allows a dynamic change of windows and levels parameters, besides the measurement of attenuation coefficients on regions of interest, which may improve the identification and characterization of the adipose material. Despite the absence of comments on this point on recent reviews(8), some of the advantages of CT include multiplanar reformatation that, although it is not essential for the diagnosis, this resource may refine the presentation of findings, facilitating the analysis of adipose tissues distribution both by radiologists and nonradiologists (Figure 2). The utilization of CT allows the investigator to rule out relevant differential diagnosis such as lymphoma and metastatic lymph node involvement. Also, it allows the tumor staging in cases where multiple symmetric lipomatosis is associated with malignant disease, particularly, squamous cell carcinoma of upper airways resulting from alcoholism and smoking whose association is frequently observed(9). Sonographic findings of lipomatosis are typical. However, despite the frequent utilization of ultrasonography in the investigation of neck masses, measurements of density by CT provide a higher diagnostic fidelity(6). MRI findings usually overlap with CT findings, but it is important to highlight that MRI is a more expensive and generally less available method(9). Despite the relatively low incidence of Madelung's disease, radiologists should know the characteristic imaging findings of this condition in order to be able to promptly achieve a correct diagnosis, ruling out overlap with other conditions and providing appropriate information for the required clinical management of the disease. REFERENCES 1. Feliciani C, Amerio P. Madelung's disease: inherited from an ancient Mediterranean population? N Engl J Med. 1999;340:1481. 2. Landis MS, Etemad-Rezai R, Shetty K, et al. Case 143: Madelung disease. Radiology. 2009;250:9514. 3. Josephson GD, Sclafani AP, Stern J. Benign symmetric lipomatosis (Madelung's disease). Otolaryngol Head Neck Surg. 1996;115:1701. 4. Ramos GHA, Trevizan GL, Pepe ES. Doença de Madelung. Rev Bras Otorrinolaringol. 2002;68:58790. 5. Murphey MD, Carroll JF, Flemming DJ, et al. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:143366. 6. Vieira MV, Grazziotin RU, Abreu M, et al. Lipomatose simétrica múltipla (doença de Madelung): relato de um caso. Radiol Bras. 2001;34:11921. 7. Bulum T, Duvnjak L, Car N, et al. Madelung's disease: case report and review of the literature. Diabetologia Croatica. 2007;36:2530. 8. Vidal MGC, Haygert CJP, Zagoury AR, et al. Doença de Madelung: relato de caso e revisão da literatura. Radiol Bras. 2010;43:2756. 9. Souza RP, Paes Junior AJO, Rapoport A. Doença de Madelung (lipomatose cervical benigna simétrica): relato de dois casos. Radiol Bras. 2003;36:1212. 1. MD, Resident of Radiology, Instituto Dr. José Frota, Fortaleza, CE, Brazil. 2. PhD, MD, Radiologist, Hospital Geral Dr. César Cals (HGCC) SESA, Fortaleza, CE, Brazil. Mailing Address: Dra. Ligia Persici Rodrigues Rua Pedro Rufino,100, 802C, Varjota Fortaleza, CE, Brazil, 60175-100 E-mail: ligia_persici@hotmail.com Received June 19, 2011. Accepted after revision October 29,2011. Study developed at the Imaging Center of Hospital Geral Dr. César Cals (HGCC) SESA, Fortaleza, CE, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554