Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 2 - Mar. / Apr. of 2012
Vol. 45 nº 2 - Mar. / Apr. of 2012
|
CASE REPORT
|
|
Breast metastasis from ovarian carcinoma: a case report and literature review |
|
|
Autho(rs): Bruno Lima Moreira1; Eduardo Nóbrega Pereira Lima2; Almir Galvão Vieira Bitencourt1; Emanuel Rafael Dantas1; Juliana Alves de Souza3; Elvira Ferreira Marques4 |
|
|
Keywords: Ovarian carcinoma; Breast metastasis; Imaging findings. |
|
|
Abstract: INTRODUCTION
Primary ovarian carcinoma rarely originates breast metastasis and there are few cases reported in the literature(1). Only about 2% of malignant neoplastic breast lesions are of secondary origin and, from a clinical and radiological point of view, they may mimic both primary benign and malignant tumors(2). Most commonly, metastatic lesions to the breast originate from primary contralateral breast tumors. However, among extramammary solid tumors, malignant melanoma, lymphoma, lung cancer, ovarian carcinoma, soft tissue sarcoma, gastrointestinal and genitourinary tumors are the ones which most frequently metastasize pato the breasts(3). In fact, according to a study developed with 4.051 patients with malignant breast lesions, only 0.07% of them presented metastasis to breast originating from ovarian tumors(1,4). The authors report the case of a patient with ovarian carcinoma who progressed with breast metastasis after about eight years from the initial diagnosis, and present a literature review on the subject with emphasis on imaging findings. CASE REPORT A female, white, 64-year-old, G1P1 patient who had menarche at 12 years and menopause at 50 years of age, former user of oral contraceptive drugs (during 15 years) and hormone replacement therapy (during 10 years), former smoker with family history of breast cancer (maternal grandmother and cousins) was submitted to surgery and chemotherapy for ovarian serous papilliferous adenocarcinoma. After the initial therapy, the patient presented locoregional and distant metastases. Eight years after the diagnosis, the patient presented a palpable mass in her left breast in association with flogistic signs on the skin. Initially, the patient was treated with antibiotic therapy, presenting improvement of the flogistic signs, but without regression of the breast mass. Then, the patient was submitted to imaging studies. Mammography (Figure 1) revealed the presence of a circumscribed mass isodense to fibroglandular tissue in the superolateral quadrant of the left breast, measuring 14 × 10 mm. Breast ultrasonography (Figure 2) demonstrated a complex cyst with solid components and thickened septa located in the superolateral quadrant of the left breast, peripherically to the papilla, measuring 13 × 8 mm, in an area of palpation at physical examination. Positron emission computed tomography (PET/CT) (Figure 3) demonstrated anomalous concentration of fluorodeoxyglicose-18F (18F-FDG) in the left breast mass, with maximum standardized uptake value (SUV) of 4.90, and also in other extramammary sites. 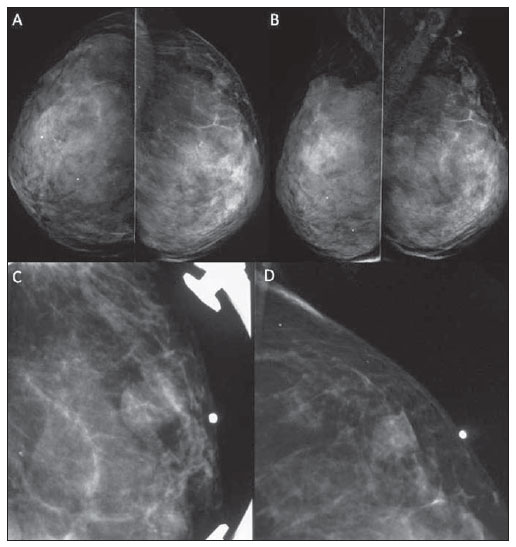 Figure 1. Mammography demonstrating a circumscribed mass isodense to fibroglandular tissue located in the superolateral quadrant of the left breast, measuring 14 × 10 mm. A: Craniocaudal view. B: Mediolateral oblique view. C,D: Absolute lateral view (C) and localized compression of the region of interest on the left breast (D) (metal marker on the skin indicating a palpable mass). 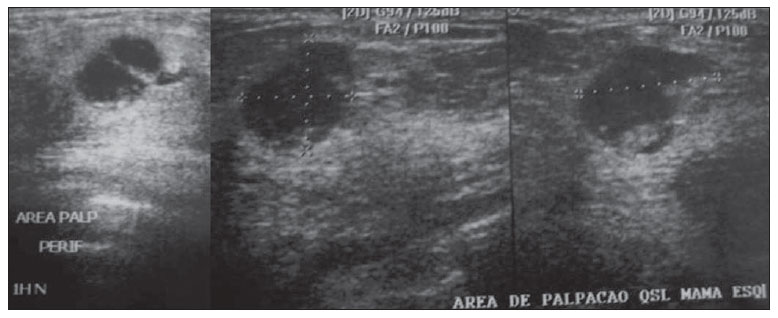 Figure 2. Breast ultrasonography demonstrating a complex cyst with solid components and thickened septa located in the superolateral quadrant of the left breast, peripherically to the papilla, measuring 13 × 8 mm, in a region of palpation at physical examination. 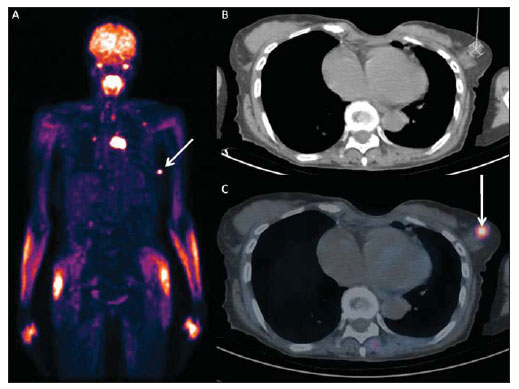 Figure 3. PET/CT image revealing anomalous uptake of 18F-FDG on a mass in left breast (arrow) with maximum SUV = 4.90 and also in other extramammary sites. A: Metabolic whole body image. B: Axial CT image at the level of the breast mass. C: Fusion PET/CT axial image at the level of the breast mass. After fine needle aspiration biopsy of the breast mass indicating the presence of neoplastic cells, the investigation was pursued with US-guided percutaneous core needle biopsy whose microscopy results were compatible with invasive carcinoma. Immunohistochemical analysis (positive cytocheratin 7; positive CA 125; negative mammoglobulin; negative BRST-2; positive WT1) led to the diagnosis of metastasis from ovarian carcinoma. Then, the patient progressed with palliative radiotherapy and chemotherapy, dying about two years after the diagnosis of breast metastasis. DISCUSSION In the presence of breast lesion in ovarian carcinoma patients, the differentiation between benign and malignant lesions is required. In case of a malignant lesion, it is necessary to know whether the lesion is primary or secondary since the treatment and prognosis differ according to the nature or the lesion(13,5). Frequently, imaging studies demonstrate metastatic lesions to the breast as dense, circumscribed and noncalcified masses. However, as a function of the presence of psamomatous bodies associated with some ovarian tumors, microcalcifications may be seen in cases of ovarian metastasis to the breast(1). But such a differentiation may be difficult, considering that metastases to the breast generally do not present specific imaging features(6). Anyway, like in the present case, the tumor origin must be investigated by means of anatomopathological analysis and taking advantage of the usefulness of immunohistochemical analysis in the differentiation of such lesions(7). PET/CT can significantly change the assessment of the disease extent in ovarian cancer patients including cases of recurrence , and change the treatment to be adopted. The positive predictive value of this method is 8998% for cases os ovarian cancer recurrence, with higher sensitivity for detecting extrapelvic lesions(8). However, in cases of breast lesions, PET/CT does not exclude the necessity of biopsy, since this imaging method does not allow the differentiation between primary and secondary malignant lesions. Once the origin of a breast lesion is confirmed as metastasis from ovarian cancer, the disease must be considered as systemic, and palliative treatment must be adopted, avoiding unnecessary surgical procedures( 13,5,6). According to some studies in the literature, the survival time of patients with breast metastasis from ovarian carcinoma is most of times less than one year(1). REFERENCES 1. Klein RL, Brown AR, Gomez-Castro CM, et al. Ovarian cancer metastatic to the breast presenting as inflammatory breast cancer: a case report and literature review. J Cancer. 2010;1:2731. 2. Garza-Guajardo R, Mendez-Olvera N, Flores- Gutierrez JP, et al. Fine needle aspiration biopsy diagnosis of metastatic neoplasms of the breast. A three-case report. Cytojournal. 2005;2:17. 3. Akçay MN. Metastatic disease in the breast. Breast. 2002;11:5268. 4. Micha JP, Goldstein BH, Epstein HD, et al. Ovarian cancer metastatic to the breast. Gynecol Oncol. 2006;102:38690. 5. Özsaran AA, Dikmen Y, Terek MC, et al. Bilateral metastatic carcinoma of the breast from primary ovarian cancer. Arch Gynecol Obstet. 2000;264:1667. 6. Bartella L, Kaye J, Perry NM, et al. Metastases to the breast revisited: radiological-histopathological correlation. Clin Radiol. 2003;58:52431. 7. Lee AH. The histological diagnosis of metastases to the breast from extramammary malignancies. J Clin Pathol. 2007;60:133341. 8. Prakash P, Cronin CG, Blake MA. Role of PET/CT in ovarian cancer. AJR Am J Roentgenol. 2010;194:W46470. 1. MDs, Residents of Radiology and Imaging Diagnosis, Department of Imaging, Hospital A. C. Camargo, São Paulo, SP, Brazil. 2. PhD, Nuclear Physician, Head of the Unit of Nuclear Medicine and PET/CT, Department of Imaging, Hospital A. C. Camargo, São Paulo, SP, Brazil. 3. MD, Radiologist, Assistant, Unit of Mammography, Department of Imaging, Hospital A. C. Camargo, São Paulo, SP, Brazil. 4. MD, Radiologist, Head of the Unit of Mammography, Department of Imaging, Hospital A. C. Camargo, São Paulo, SP, Brazil. Mailing Address: Dr. Bruno Lima Moreira Rua Doutor Jambeiro Costa, 57, ap. 34, Liberdade São Paulo, SP, Brazil, 01509-030 E-mail: limamoreiramed@gmail.com Received September 16, 2011. Accepted after revision October 28, 2011. Study developed at Department of Imaging, Hospital A. C. Camargo, São Paulo, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554