Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 6 - Nov. / Dec. of 2010
Vol. 43 nº 6 - Nov. / Dec. of 2010
|
ORIGINAL ARTICLE
|
|
Analysis of three-dimensional power Doppler sonography reproducibility in the assessment of fetal brain circulation* |
|
|
Autho(rs): Antonio Fernandes Moron1; Hérbene José Figuinha Milani2; Enoch Quinderé de Sá Barreto3; Edward Araujo Júnior4; Karina Krajden Haratz2; Liliam Cristine Rolo2; Luciano Marcondes Machado Nardozza5 |
|
|
Keywords: Reproducibility of results; Prenatal ultrasonography; Fetal brain flow; Power Doppler; Threedimensional sonography. |
|
|
Abstract: INTRODUCTION
Both the fetal and uteroplacental circulations have been exhaustively studied with the objective of evaluating the fetal hemodynamics in the physiological and pathological processes during pregnancy(1). In this context, the evaluation of the fetal brain vascularization and blood flow is extremely relevant, considering that perfusional deficits in this territory may be determinant in a poor prognosis for the development of the central nervous system and even for the fetal welfare(2). Ultrasonography is a noninvasive diagnostic method for evaluating the cerebral blood flow, and indirectly inferring the fetal oxygenation status. Presently, in obstetrics, 2D color Doppler and power Doppler ultrasonography are the two main sonographic techniques utilized for evaluating vascularization and blood flow. Two-dimensional color Doppler can analyze the changes in blood flow waves and has been utilized as the main noninvasive diagnostic method in the evaluation of fetal circulation and blood flow. This method allows the evaluation of the fetal brain oxygenation status through the measurement of the blood flow waves velocity. It is utilized as a reference in the study of the cerebral blood flow in the middle cerebral artery (MCA), considering the facility for identification and high reproducibility of the method(3). Although 2D color Doppler can provide relevant clinical data on the fetal hemodynamics, this method presents limitations inherent to its lower sensitivity to detect low-velocity flows and angle dependence, besides being subject to aliasing effect(4). Power Doppler evaluates the amplitude of the received signals, indicating the number of moving cells, so this method is more sensitive for evaluating small vessels and low-velocity flows, allowing the detection of minimal changes in the blood flow(5). Such characteristic is extremely relevant in the evaluation of low-resistance vessels(6). With the arrival of 3D ultrasonography, power Doppler started being utilized for 3D analysis of blood flow and vessels. However, the first studies with this new technique included only a qualitative evaluation by means of 3D reconstruction of the vascular structure of a region of interest (ROI), without quantifying the vascularization and the blood flow of this territory(7). Pairleitner et al.(8), in an analysis of adnexal masses, have described a new technique in an attempt to quantify blood flow and vascularization by means of 3D ultrasonography: 3D power Doppler. Based on the analysis of voxels (the smallest units in a 3D image), of the gray-scale and color and size parameters of a previous selected cube (volume of interest) plotted on a histogram, the authors have created three indices to measure vascularization (vascularization index VI), blood flow (flow index FI), or both (vascularization-flow index VFI), as follows: VI measures the percentage of color voxels in total voxels within the ROI, and estimates the number of blood vessels in the tissues expressed in percentage; FI represents the weighted color value of all the color voxels and shows the mean blood flow signal intensity; and VFI corresponds to weighted color value of all the color voxels and gray scale, representing the behavior of the other two indices. Up to the present moment, the fetal brain circulation has been traditionally based on the middle cerebral artery pulsatility and resistance indices measured by means of 2D ultrasonography(9). Such indices indicate vascular impedance and do not estimate changes in the blood flow within small vessels responsible for variations in the cerebral tissue perfusion(10). For this reason the utilization of 3D power Doppler in the evaluation of the fetal brain circulation is particularly relevant because of the small diameter of blood vessels in this territory, besides being an important tool in the study of fetuses with growth restriction in an attempt to achieve an earlier prediction of the mechanism involved in the fetal hemodynamics centralization. The present study was aimed at evaluating the intra- and interobserver reproducibility of 3D power Doppler in the study of the fetal brain vascularization and blood flow, considering the MCA territory as ROI. MATERIALS AND METHODS A cross-sectional, observational study was developed with 20 randomly selected healthy pregnant women between 26 and 34 gestational weeks. The study was approved by the Committee for Ethics in Research of Universidade Federal de São Paulo (Unifesp) and all the women participating in this research signed a term of free and informed consent. All the sonographic examinations and 3D volumes acquisition were performed by a single observer with three-year experience in 3D ultrasonography, with a Voluson 730 Expert unit (GE Medical Systems; Kretz, Zipf, Austria), equipped with a multi-frequency volumetric, convex transducer (4.07.0 MHz) and with integrated 4D View version 9.0 software (GE Medical Systems; Kretz, Zipf, Austria) for storage and manipulation of 3D ultrasonography data. Initially, a conventional evaluation was performed with 2D ultrasonography for demonstrating fetal positioning and presentation, heart beats, fetal biometrics, fetal weight estimation and morphological study, placental positioning and grade, amniotic fluid, and conventional Doppler velocimetry of uterine, umbilical and middle cerebral arteries. The study of the fetal brain vascularization by means of 3D power Doppler started with the identification of the circle of Willis with the aid of 2D color Doppler. Subsequently, the 3D power Doppler angio-mode was activated with three-dimensional comprising the whole circle of Willis. In order to achieve an appropriate 3D volume acquisition, the scan was performed in the absence of fetal movements and with the pregnant patient momentaneously holding her breath. The following presets were utilized for volumes acquisition: penetration frequency (low), power (1), gain (50), frame rate (2), sensitivity (15), density (activated), balance (16), scale (0.9 kHz) and filter (1). After volumes acquisition, the 3D image was presented in three orthogonal planes perpendicular to each other, the so called multiplanar mode. Subsequently, the acquired 3D volumes were twice evaluated by the main observer at different moments with an interval of less than 24 hours, for the purpose of intraobserver variability analysis. A second observer also with three-year experience in 3D ultrasonography, performed a third evaluation of the 3D volumes for determining the interobserver variability. The initial measurements were not known by the main observer at the moment of the second evaluation, and the second observer did not know the values previously obtained by the main observer. The analysis of the 3D volumes for calculation of the 3D power Doppler indices by both the observers was performed as follows: initially, the three planes were explored to localize the region with a major vascularization within the ROIs, taking the axial plane as a reference. The ROI was the MCA territory closest to the transducer. The Virtual Organ Computer-aided AnaLysis (VOCAL) was selected for allowing the manual determination of the area in the fetal brain where the 3D power Doppler vascular indices were analyzed. The measurement calipers were positioned on the origin and on the apex of the middle cerebral artery closest to the transducer. Subsequently, the sphere mode was selected to define the contours of the previously calibrated region of interest. Once the ROI was appropriately included in the brain tissue sphere, the VOCAL Shell Histogram key was selected to automatically calculate all the 3D power Doppler vascular indices (VI, FI and VFI) (Figure 1). This technique is similar to the one proposed by Mercé et al.(11) for the study of placental vascularization denominated vascular biopsy. 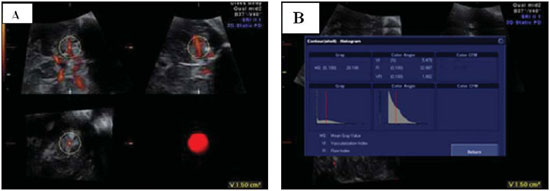 Figure 1. A: VOCAL sphere mode selecting the anterior middle cerebral artery territory. B: Selecting the VOCAL Shell Histogram key, with automated calculation of 3D power Doppler indices (VI, FI and VFI). The data were stored on an Excel 2003 (Microsoft; Redmond, WA, USA) work-sheet and then analyzed by specific statistical software, SPSS for Windows version 15.0 (SPSS Inc.; Chicago, IL, USA). Reproducibility (the property of a test presenting equivalent results in different occasions with a single observer intraobserver variability , or between different observers interobserver variability) was calculated by means of the intraclass correlation coefficient (ICC) and Bland-Altman plots(12). The significance level was set at 5% for all the tests (p < 0.05). RESULTS The present study evaluated 20 pregnant women in the age range between 25 and 38 years (mean, 31 years). Gestational age ranged between 26 and 33 6/7 weeks (mean, 29.8 weeks). The number of previous labors ranged from 0 to 4 (mean, 2.1 labors). The descriptive statistics regarding vascular indices obtained through 3D power Doppler for the MCA territory are shown on Table 1. 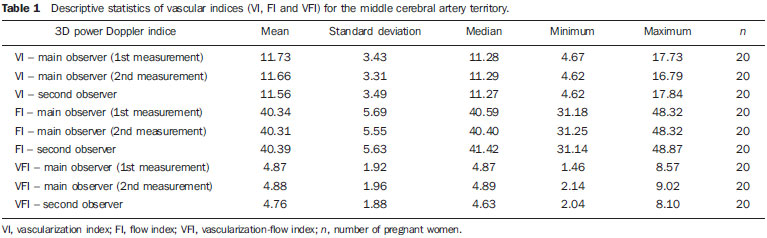 The intraobserver variability in the evaluation of the MCA territory demonstrated an ICC > 0.90 for the three indices, with FI demonstrating the best rate of agreement (ICC = 0.999) (Table 2). According to the Bland-Altman plots, the mean differences in the intraobserver reproducibility were the following: VI = 0.30 (limits of agreement: 8.4 to 9.0), FI = 0.03 (limits of agreement: 1.43 to 1.49) and VFI = 0.10 (limits of agreement: 9.4 to 9.2) (Figure 2). 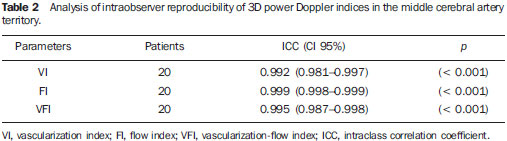 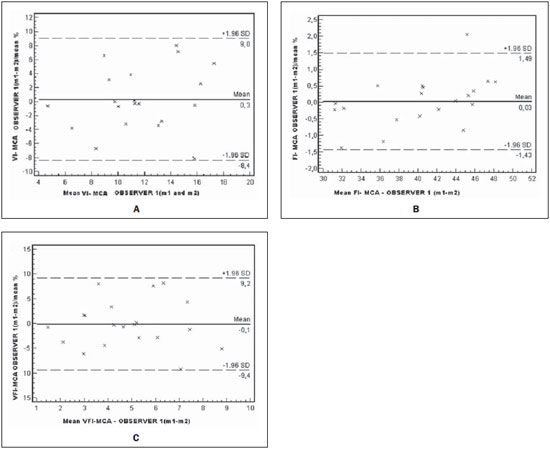 Figure 2. Differences of measurements performed by a single observer plotted against the average of differences and 1.6 standard deviation for VI (A), FI (B) and VFI (C). The interobserver variability in the evaluation of the MCA territory demonstrated an ICC > 0.90 for the three indices, with FI demonstrating the best rate of agreement (ICC = 0.999) (Table 3). Mean differences in the interobserver reproducibility were the following: VI = 1.16 (limits of agreement: 9.1 to 12.4), FI = 0.16 (limits of agreement: 1.85 to 1.53) and VFI = 2.1 (limits of agreement: 7.5 to 11.8) (Figure 3). 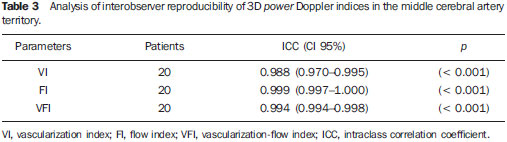 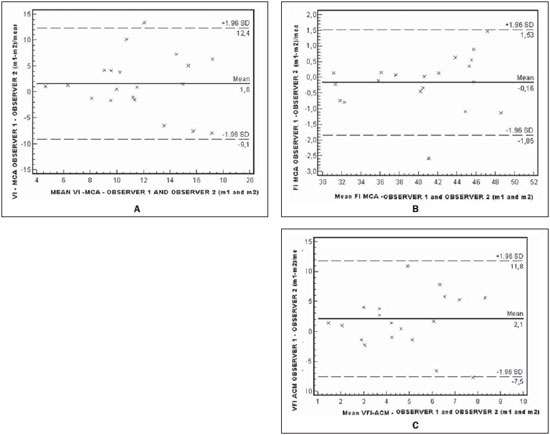 Figure 3. Differences between measurements performed by two observers plotted against the average of differences and 1.6 standard deviation for VI (A), FI (B) and VFI (C). DISCUSSION With technological developments in the field of imaging diagnosis, new methods have been introduced to provide additional information on vascularization and blood flow in human organs and structures. Three-dimensional power Doppler is a recent technology that allows to objectively quantifying vascularization and blood flow in specific structures by means of the analysis of three indices: VI, FI, and VFI(8). Several studies have utilized this method to evaluate placental vascularization(11) and fetal organs(2,6,13,14). The first study approaching the evaluation of fetal brain vascularization by 3D power Doppler has been developed by Chang et al.(1). These authors have evaluated 155 healthy pregnant women between 21 and 40 gestational weeks, considering the circle of Willis as ROI, utilizing the manual VOCAL method, and have demonstrated a significant increase in VI, FI and VFI with the progression of the gestational age and with fetal biometrical parameters. The intraobserver variability was evaluated in only 20 cases which were randomly selected among the 155 pregnant women, with high ICC for the three indices [VI (ICC = 0.95), FI (ICC = 0.93), VFI (ICC = 0.95)]. Bartha et al.(15) have also studied the 3D power Doppler reproducibility in the evaluation of fetal brain vascularization, considering the whole fetal brain as ROI and utilizing the sphere mode of the VOCAL method. These authors have demonstrated a good intraobserver reproducibility (ICC > 0.85 for VI, FI and VFI) and good interobserver reproducibility for VI (ICC = 0.92) and VFI (ICC = 0.88), with lower value for FI (ICC = 0.67). Our study demonstrated good intra- and interobserver variability for 3D power Doppler in the evaluation of fetal brain vascularization, with ICC > 0.90 for VI, FI and VFI, in agreement with the findings reported by Chang et al.(1) and Bartha et al.(15). However, we observed a better interobserver agreement for FI (ICC = 0.999) as compared with the value reported by Bartha et al.(15) (ICC = 0.67). This is probably due to the fact that the authors studied only the MCA territory, while Bartha et al.(15) considered the whole fetal brain as ROI. In fact, we have chosen the MCA as ROI, because it is the main branch of the internal carotid artery, being responsible for 80% of the blood flow towards the cerebral hemispheres. It is known that the circle of Willis is the main vascular structure responsible for the blood flow distribution to the fetal brain(1). However, considering the high sensitivity of 3D power Doppler, with the vascular indices calculated by this method being subject to depth-related sound attenuation(16), it becomes difficult to evaluate the whole circle of Willis structure, particularly at more advanced gestational ages because of the fetal movements and the mothers respiration. For this reason, the authors have opted for studying only the MCA territory closer to the transducer, so minimizing the effects from sound attenuation and imaging artifacts. We utilized a technique similar to the one described by Mercé et al.(11) in the evaluation of placental vascularization, called vascular biopsy. Such method consists in utilizing the VOCAL software to determine a sphere in the ROI as a volume representing the whole structure and, based on the histogram, calculating the VI, FI and VFI. Another study developed by the same group has demonstrated a good reproducibility with this technique, resulting in ICC > 0.85 for all the 3D power Doppler indices(17). We have opted to utilize the VOCAL method sphere mode, since it reduces the variability associated with the manual method(17), besides allowing a review of all the sphere planes, so confirming either the presence or absence of the vessel in all of them(6). Likewise in the present study, Nardozza et al.(6), applying the technique similar to vascular biopsy proposed by Mercé et al.(11), and considering the MCA territory as ROI, have evaluated 90 healthy pregnant women between 26 and 35 gestational weeks, and have demonstrated a poor correlation between VI, FI and VFI and gestational age, concluding that this technique is practical, rapid and easy to perform. However, the reproducibility of such technique has not been evaluated by these authors. Based on volumes previously collected and stored by a single observer, we tested the intra- and interobserver reproducibility of the method. Therefore, the reproducibility of the whole procedure from the volume acquisition has not been evaluated. According to Järvelä et al.(18), there are two possible ways to analyze the reliability involving the utilization of the 3D technique: by 3D volume acquisition and through calculation of the volume after contour definition by means of the VOCAL method (stored volumes), so the reliability in the 3D volume acquisition is directly related to the confidence level of an accurate delineation of the volume to be calculated(19). Additionally, according to Raine-Fenning et al.(20), the data acquisition is much more subject to results uncertainty than a series of measurements of any data, particularly in Doppler velocimetric studies. Several studies have evaluated the reproducibility of measurements with the VOCAL software, including 3D power Doppler indices, based on data collected by a single observer and that later were analyzed by different observers(1,15,1821). Based on such studies, we consider their findings as relevant and reliable. CONCLUSION The cerebral circulation can be evaluated by 3D power Doppler, with the vascular biopsy technique to study the MCA. Three-dimensional power Doppler has shown to be a practical and easy method in the assessment of fetal brain blood flow, with good intra- and interobserver reproducibility. REFERENCES 1. Bell JG, Ludomirsky A, Bottalico J, et al. The effect of improvement of umbilical artery absent end-diastolic velocity on perinatal outcome. Am J Obstet Gynecol. 1992;167(4 Pt 1):101520. 2. Chang CH, Yu CH, Ko HC, et al. Three-dimensional power Doppler ultrasound for the assessment of the fetal brain blood flow in normal gestation. Ultrasound Med Biol. 2003;29:12739. 3. Wladimiroff JW, VanDen Wijngaard JA, Degani S, et al. Cerebral and umbilical arterial blood flow velocity waveforms in normal and growth-retarded pregnancies. Obstet Gynecol. 1987;69:7059. 4. Yu CH, Chang CH, Ko HC, et al. Assessment of placental fractional moving blood volume using quantitative three-dimensional power Doppler ultrasound. Ultrasound Med Biol. 2003;29:1923. 5. Rubin JM, Bude RO, Carson PL, et al. Power Doppler US: a pontentially useful alternative to mean frequency-based color Doppler US. Radiology. 1994;190:8536. 6. Nardozza LMM, Araújo Júnior E, Simioni C, et al. Evolution of 3-D power Doppler indices of fetal brain in normal pregnancy. Ultrasound Med Biol. 2009;35:5459. 7. Chaoui R, Kalache KD, Hartung J. Application of three-dimensional power Doppler ultrasound in prenatal diagnosis. Ultrasound Obstet Gynecol. 2001;17:229. 8. Pairleitner H, Steiner H, Hasenoehrl G, et al. Three-dimensional power Doppler sonography: imaging and quantifying blood flow and vascularization. Ultrasound Obstet Gynecol. 1999;14:13943. 9. Konje JC, Bell SC, Taylor DJ. Abnormal Doppler velocimetry and blood flow volume in the middle cerebral artery in very severe intrauterine growth restriction: is the occurrence of reversal of compensatory flow too late? BJOG. 2001;108:9739. 10. Hernandez-Andrade E, Jansson T, Figueroa-Diesel H, et al. Evaluation of fetal regional cerebral blood perfusion using power Doppler ultrasound and the estimation of fractional moving blood volume. Ultrasound Obstet Gynecol. 2007;29:55661. 11. Mercé LT, Barco MJ, Bau S, et al. Assessment of placental vascularization by three-dimensional power Doppler vascular biopsy in normal pregnancies. Croat Med J. 2005;46:76571. 12. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:30710. 13. Chang CH, Yu CH, Ko HC, et al. Assessment of normal fetal liver blood flow using quantitative three-dimensional power Doppler ultrasound. Ultrasound Med Biol. 2003;29:9439. 14. Chang CH, Yu CH, Ko HC, et al. Quantitative three-dimensional power Doppler sonography for assessment of the fetal renal blood flow in normal gestation. Ultrasound Med Biol. 2003;29:92933. 15. Bartha JL, Moya EM, Hervías-Vivancos B. Three-dimensional power Doppler analysis of cerebral circulation in normal and growth-restricted fetuses. J Cereb Blood Flow Metab. 2009;29:160918. 16. Raine-Fenning NJ, Welsh AW, Jones NW, et al. Methodological considerations for the correct application of quantitative three-dimensional power Doppler angiography. Ultrasound Obstet Gynecol. 2008;32:1157. 17. Mercé LT, Barco MJ, Bau S. Reproducibility of the study of placental vascularization by three-dimensional power Doppler. J Perinat Med. 2004;32:22833. 18. Järvelä IY, Sladkevicius P, Tekay AH, et al. Intraobserver and interobserver variability of ovarian volume, gray-scale and color flow indices obtained using transvaginal three-dimensional power Doppler ultrasonography. Ultrasound Obstet Gynecol. 2003;21:27782. 19. Duin LK, Willekes C, Vossen M, et al. Reproducibility of fetal renal pelvis volume measurement using three-dimensional ultrasound. Ultrasound Obstet Gynecol. 2008;31:65761. 20. Raine-Fenning NJ, Campbell BK, Clewes JS, et al. The reliability of virtual organ computer-aided analysis (VOCAL) for the semiquantification of ovarian, endometrial and subendometrial perfusion. Ultrasound Obstet Gynecol. 2003;22:6339. 21. Bortoletti Filho J, Nardozza LMM, Araujo Júnior E, et al. Reprodutibilidade interobservador dos índices vasculares do Doppler de amplitude tridimensional do embrião entre 7 e 10 semanas e 6 dias de gestação. Radiol Bras. 2010;43:1438. 1. Private Docent, Titular Professor, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. 2. Masters, MDs, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. 3. MD, Fellow degree, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. 4. PhD, Associate Professor, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. 5. Private Docent, Associate Professor, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. Mailing Address: Dr. Edward Araujo Júnior Departamento de Obstetrícia da Universidade Federal de São Paulo (Unifesp) Rua Napoleão de Barros, 875, Vila Clementino São Paulo, SP, Brazil, 04024-002 E-mail: araujojred@terra.com.br Received July 17, 2010. Accepted after revision October 7, 2010. * Study developed at the Division of Three-dimensional Ultrasonography, Department of Obstetrics Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554