Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 4 - July / Aug. of 2010
Vol. 43 nº 4 - July / Aug. of 2010
|
ORIGINAL ARTICLE
|
|
Comparative study between computed tomography and bronchoscopy in the diagnosis of lung cancer |
|
|
Autho(rs): Christopher Oliveira1; António Saraiva2 |
|
|
Keywords: Lung cancer; Imaging diagnosis; Bronchoscopy. |
|
|
Abstract: INTRODUCTION
Lung cancer epidemiology Lung cancer represents one of the mostfrequent neoplasias worldwide, accountingfor the highest rate of deaths caused by malignancy in both men and women. In theUSA, lung cancer is the main cause ofdeath by neoplasia (representing about28% of deaths by neoplasia/year). In Portugal, the estimated incidence is 34 casesper 100,000 men, and 28 cases per 100,000women. The highest incidence rate is observed in the age range from 55 to 65 years.Despite the recent therapeutic developments, the five-year survival rates amongthese patients remain as low as about 13%(1-4). Lung cancer etiology It was long ago that tobacco consumption was established as the main etiological factor in lung cancer. Smoking individuals present a 22-time higher risk for death by this disease than non-smoking individuals, and the strongest association with tobacco consumption has been observed in cases of small-cell lung cancer, squamous-cell carcinomas and large-cell lung carcinomas. Passive smoking is an increasingly relevant risk factor, representing 3% to 5% of all cases of lung cancer(3,5,6). It is important to note that tobacco consumption is not the sole cause of lung cancer; other factors may be associated, affecting the disease incidence: exposure to arsenic, chromium, nickel and asbestos, cicatricial lesions of tuberculosis, bullous emphysema, and familial history of lung cancer(2). Clinical presentations It should be highlighted that more than 90% of patients with lung cancer are asymptomatic at presentation, with clinical findings resulting from local, regional, metastatic or systemic effects of the tumor. Generally, the main symptom is persistent cough. The incidence of hemoptysis achieves 27-57%. Massive hemoptysis is less frequently found. Additionally, dyspnea and paraneoplastic syndromes constitute the main symptoms in cases where the tumor is limited to the lung(3,5-9). The presence of chest pain, hoarseness, brachial plexus neuropathies, Horner's syndrome, dysphagia and pericardial tamponade is suggestive of mediastinal or chest wall invasion(3). Main histological types of lung cancer In the present study, the description of histological types will be based on the criteria of the World Health Organization (WHO) for histological classification of lung cancer(9). The division of lung cancer into nonsmall cell lung carcinoma (NSCLC) and small cell lung carcinoma (SCLC) is crucial for the therapeutic planning(3,4). The four main histological types include: adenocarcinoma, squamous cell carcinoma, SCLC and large-cell carcinoma. SCLC is considered as a histological subtype with characteristics including an aggressive clinical behavior with fast cell proliferation, early metastatization and, nearly always, presentation at diagnosis as nonresectable disease(3,5). Lung cancer diagnosis The diagnostic evaluation of this disease has two main objectives: the definition of the pathological type of tumor and staging of the disease(7,10). Chest computed tomography (CT) plays a relevant role in the determination of presence and extent of lung cancer, demonstrating the size and site of the tumor. However, this method presents some limitations such as high cost, utilization of ionizing radiation, contrast agent nephrotoxicity, besides the necessity of further procedures to confirm the diagnosis(2,11). The CT indispensability in the study of lung cancer is associated with the obligatoriness of endoscopy of the respiratory tract with flexible endoscope. Endoscopic signs of cancer are quite variable, from a simple bright loss in a small region of the bronchial mucosa to a typical vegetative mass. Classically, three types of typical lesions or direct signs of tumor are taken into consideration: mass, infiltration and obstruction. The techniques associated with bronchofibroscopy include bronchial wash and brush cytology and bronchial biopsy(5,12-17). Lung cancer staging The staging analysis was based on the most recent revision of the TNM system dated of 1997. The staging is aimed at dividing cancer patients into subgroups to define their prognosis and to determine the therapeutic options. It is important to note that imaging methods play an essential role in the staging and follow-up of patients with lung cancer(2,11,18). The TNM system comprises several stages (IA, IB, IIA, IIB, IIIA, IIIB, IV) according to characteristics regarding: T - evaluation of the primary tumor; N - evaluation of lymph nodes involvement; M - evaluation of distant metastases(19). In the clinical practice, the traditional TNM system is not useful in the staging of SCLC, limiting the staging to "limited disease" and "extensive disease"(3,4). Lung cancer therapeutic An early diagnosis is the determining factor in the therapeutic selection. Surgery, chemotherapy and radiotherapy are the most frequently utilized types of treatment(5). The most relevant therapeutic decision is related to the tumor resectability assessment, considering that surgery is the only potentially curative treatment. The type of surgical therapy is also dependent on the tumor type, site and extent, besides the patient's age and general clinical condition. Many times a combination of two or even three treatment modalities is required(3-5,20). MATERIALS AND METHODS Study location and population The present study was developed in the Unit of Pneumology of Hospital Distrital da Figueira da Foz, Coimbra, Portugal, in the period between January and July/2009, evaluating the clinical records of 70 patients. The study population included patients referred to the Unit of Pneumology along a four-year period (January-2003 to January-2007) and submitted to CT and bronchoscopy for suspicion of lung cancer, confirmed or not by histopathological study. No other exclusion/inclusion criteria were considered. Age, gender, smoking habits, histological types, staging and therapeutic options were also evaluated. Search method and data analysis A data record form was prepared for data collection and subsequent analysis. The data used in the present study were collected in the patients' clinical records. The present study was developed with the collaboration of two pneumologists. Bronchoscopy and CT studies were considered as either negative or positive according to the data included in the respective reports. Bronchoscopy studies and the subsequent reports preparation were performed by a pneumologist. A radiologist performed the chest CT studies and prepared the respective reports. On average, a two-day time interval was observed between the performance of CT studies and bronchoscopy. It is important to mention that chest, upper abdomen and skull CT, bronchoscopy, bone scintigraphy and mediastinoscopy were performed for the disease staging. Once the data collection was completed, the Statistical Package for the Social Sciences (SPSS) v17 was utilized for appropriate data processing and analysis, allowing an accurate inference about the results of the present study. Ethical considerations The present investigation was fully compliant with the WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. Such declaration is worldwide recognized as thebasic principles to be followed in medicalresearch involving human subjects, including the respect for the human subject, besides the Principles of Beneficence and Justice. Thus patients were guaranteed their anonymity as well as the confidentiality of their clinical information. RESULTS In the present study, clinical records of 70 patients assisted in the Unit of Pneumology were analyzed. The patients (60% men and 40% women, in the age range between 35 and 84 years, mean = 66 years) had been referred with symptoms suggestive of lung cancer and were submitted to bronchoscopy and lung CT. Among the 37 cases diagnosed with lung cancer, the mean age was 66.24 years (± 10.03), 23 were male and 14 female patients. At the time of the diagnosis, only one patient was under 45 years of age and 19 patients were aged > 70 years (Figure 1). 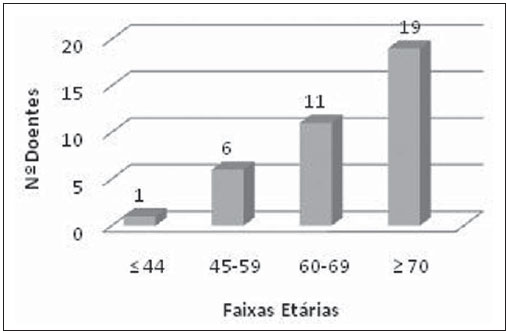 Figure 1. Distribution of cancer patients by age range. Table 1 demonstrates the sample characterization regarding smoking habits. Most of the patients smoked or had ever smoked, corresponding to 55.7% (n=39), while the number of the non-smoking ones corresponded to 44.3% of the whole study sample. It is important to note that among the women participating in the present study, none smoked neither had ever smoked (n=28). Differently, only 7.1% of the male patients did not smoke.  Distribution of lung cancer types Among the 70 patients submitted to bronchoscopy and CT, 37 presented lung cancer. Among these 37 cases, 30(80.08%) were NSCLC and 7 were SCLC (18.92%). Adenocarcinoma was the most frequent histological type observed (40.54%; n=15), followed by squamous-cell carcinoma (32.43%; n=12) and SCLC (18.92%; n=7). As far as the rarest tumors are concerned, 5.41% were large-cell carcinomas and 2.70%, carcinoid tumors (Figure 2). 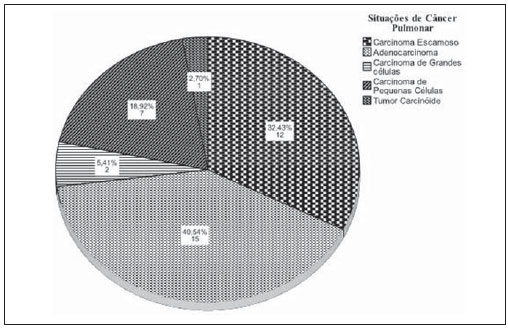 Figure 2. Histological types of lung cancer. Relation between smoking habits and presence/absence of lung cancer In spite of the fact that the statistical analysis has indicated no statistical significance (p > 0.05) in the relation between smoking habits and presence/absence of lung cancer, it is essential to mention that the majority of the patients diagnosed with lung cancer, 59.46% (n=22), smoked or had ever smoked, and 40.54% (n=15) did not smoke (Table 2). 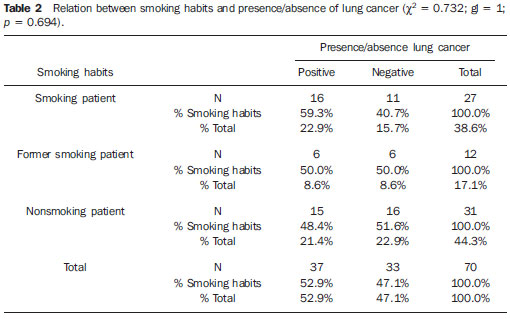 Staging In the present study, it is important to evaluate the staging in the setting of NSCLC. Figure 3 demonstrates that the majority of the patients presented with advanced stages of disease, i.e., stages IIIB (36.70%) and IV (33.30%) in a total of 70%. Eventually surgical stages correspond to 30%, with stage IB with 6.70% of cases, and stage IIIA with 23.30%.  Figure 3. NSCLC staging. Therapeutics As regards therapeutics, it is important to note that surgery was performed as first therapeutic option (Figure 4) in 8.1% of the patients. Chemotherapy alone was performed in 75.7% of the cases. In 16.2% of the cases, the patients underwent combined therapy (combined surgery-chemotherapy, surgery-radiation therapy or association of chemotherapy and radiation therapy). Radiation therapy was not performed as a first therapeutic option, although this method has been utilized in combination with chemotherapy or surgery in certain cases. It is convenient to mention that the surgeries were performed in the Unit of Chest Surgery at Centro Hospitalar de Coimbra, the chemotherapy sessions at Hospital Distrital da Figueira da Foz, and the radiation therapy sessions at Instituto Português de Oncologia de Coimbra. 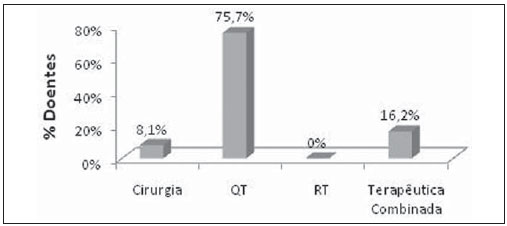 Figure 4. Lung cancer therapeutics. Relation between bronchoscopy results and presence/absence of lung cancer The statistical analysis allowed the authors to observe that the relation between bronchoscopy results and the presence/absence of lung cancer was statistically significant (p < 0.05). The kappa value 0.656 demonstrated a good rate of agreement between the obtained results. The authors observed that, among the 37 positive bronchoscopic results, 31(83.8%) corresponded to a positive diagnosis of cancer, and 6(16.2%) to a negative diagnosis of the disease. As regards the 33 negative bronchoscopic results, 27(81.8%) really corresponded to a negative diagnosis of lung cancer, and 6(18.2%) to a positive diagnosis of cancer (Table 3). In these 6 cases, the final diagnosis was achieved by means of transthoracic biopsy in 4 cases, and surgical biopsy in 2 cases. In the present study, bronchoscopy sensitivity was of 83.8%, specificity, 81.8%, and accuracy, 82.8%. False-positive results corresponded to 18.2%, and false-negative results, to 16.2%. 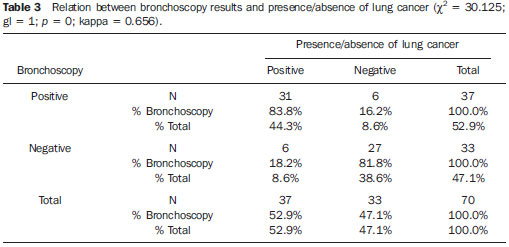 Relation between CT results and presence/absence of lung cancer The statistical analysis demonstrated that the relation between CT results and presence/absence of lung cancer was statistically significant (p < 0.05). Kappa value was of 0.451, corresponding to a weak agreement between results. The authors observed that among the 42 CT studies interpreted as positive, 30(71.4%) corresponded to a positive diagnosis of lung cancer, and 12(28.6%) corresponded to a negative diagnosis of the disease. As regards the 28 tomographic studies interpreted as negative, 21(75%) really corresponded to absence of lung cancer, while 7(25%) ended up demonstrating the presence of disease (Table 4). In these 7 cases, the final diagnosis was achieved by means of bronchial biopsy in 6 cases, and by means of transthoracic biopsy in 1 case. In the present study, the CT sensitivity was of 81.1%, specificity, 63.6%, and accuracy, 72.8%. False-positive results corresponded to 36.4% and false-negative results, to 18.9%. 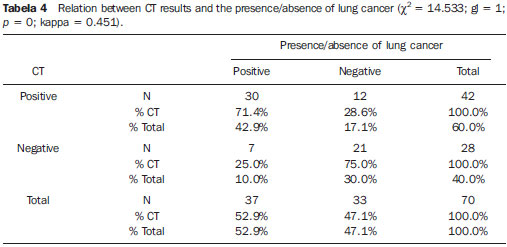 DISCUSSION The main objective of the present study was to evaluate the effectiveness of bronchoscopy and CT in the diagnosis of lung cancer. For this purpose, the authors analyzed the medical records of 70 patients referred to the Unit of Pneumology of Hospital Distrital da Figueira da Foz for suspicion of lung cancer and submitted to both diagnostic methods. Additionally, the following parameters were evaluated: patients' age, gender, staging and therapeutic options. In the present study, the mean age observed in cases of lung cancer, 66.24 years, is similar to the one reported in other larger series, both at national and international levels(21,22). Men were most affected, with 23 cases of cancer, while 14 cases were observed among women. Studies in the literature report that male individuals are most affected by lung cancer, despite the increase observed in the number of cases among women in the last decades(23,24). As already mentioned in the introduction of the present study, the smoking habit is the main factor involved in the etiology of lung cancer, but a small percentage of smoking individuals develop such disease, suggesting that the disease etiology is multifactorial(25). Such data reported in the literature may corroborate the results observed in the evaluation of the relation between smoking habits and presence/absence of lung cancer which did not demonstrate statistical significance (p > 0.05). However, it is important to note that among the cases diagnosed as lung cancer, the majority of them (59.46%) corresponded to smoking and former smoking individuals. In the present series, adenocarcinoma was the prevalent histological type. The medical literature reports a remarkable increase in the number of cases of adenocarcinomas and a corresponding decrease in the number of cases of squamous-cell carcinomas(26,27). As regards staging, the authors observed that most patients presented advanced stages of disease, IIIB and IV, in agreement with data in the literature that as a matter of fact demonstrate their highest frequency in the clinical routine(26,28). Recent studies have indicated that patients with stages III and IV present an extremely poor and limited five-year survival(28). The present study does not approach the staging of SCLC in cases of limited and extensive disease, since the authors could not collect the necessary data to analyze the subject. In the present investigation, a small number of patients - only 8.1% of cases - was submitted to surgery, while chemotherapy - with 75.7% of cases - was the most utilized therapeutics. The medical literature clearly describes the surgical therapy as critical in the treatment of lung cancer(29). However, studies report a small number of patients submitted to surgery and demonstrate that resectability criteria are met in only 20% of cases at the time of diagnosis(23,24,30). The situations observed regarding both the staging (predominance of most advanced stages of disease) and therapeutic options (small number of patients submitted to surgery) demonstrates that the late diagnosis in most of cases still poses a challenge, considering the difficulty in the achievement of an early diagnosis. Bronchoscopy is thought to be fundamental in the diagnosis of lung cancer and also in the staging and follow-up of the disease(14,31,32). This rating found in studies in the literature is corroborated by the results of the present study (sensitivity, 83.8%; specificity, 81.8%; accuracy, 82.8%). Currently, new advances in techniques associated with bronchoscopy have allowed developments to improve the diagnosis of lung cancer(31,33). The literature indicates that in more than 70% of cases, carcinomas can be detected by bronchoscopy, and the performance of such method is enhanced, provided it is associated with bronchial biopsy, bronchial wash and brush cytology(13,29,31,34). The false-negative results (16.2%) of bronchoscopy are due to the presence of peripheral lesions, particularly the smaller ones, because of the poor role played by bronchoscopy in these cases, corroborating data in the literature(15,35). Imaging methods represent an essential diagnostic tool in the evaluation of lung cancer(36). Computed Tomography plays a relevant role in the diagnosis of lung cancer, as corroborated by studies in the literature(36-38). In the present study, CT presented sensitivity of 81.1% corroborating reports in the reference literature demonstrating that as lung cancer is detected by radiological methods, ¾ of the natural history of the disease were already completed(38,39). The specificity is a result of the number of false-positive results (36.4%). This situation demonstrated by the studies referenced herein is due to the fact that radiological findings suggestive of lung cancer (leading to the rating of a CT study as positive) such as parenchymal mass with spiculated margins, microlobulations, thick-walled cavities, cavitary nodules and chest wall invasion may be observed in other diseases such as infections, pulmonary inflammatory processes, infarction and lung abscesses.(40,41). CONCLUSION Lung cancer diagnosis is essentially achieved by CT and bronchoscopic techniques. The association of bronchoscopy and CT is useful in the accurate diagnosis of lung cancer, since the occurrence of false-positive results of CT is minimized, improving the specificity of the method. On the other hand, the utilization of CT to detect the presence of peripheral lesions, which increase the incidence of false-negative results of bronchoscopy, allows a better management of patients, increasing the diagnostic accuracy. The association of these two methods, besides the discussion between pneumologists and radiologists constitute the best approach for lung cancer patients. Acknowledgements The authors would like to thank Hospital Distrital da Figueira da Foz, the Unit of Pneumology, particularly Dr. António Antunes, Director for the mentioned Unit and Dr. Manuela Lopes, for the collaboration and willingness. REFERENCES 1. Agarwal A, Ghotekar LH, Garbyal RS, et al. Evaluation of pulmonary malignancies in Kathmandu Valley and role of bronchoscopic techniques in diagnosis of such cases. JIACM. 2003;4:127-33. 2. Figueiredo L, Bento MT. Neoplasia do pulmão. In: Pisco JM, Sousa LA. Noções fundamentais de imagiologia. Lisboa: Lidel-Edições Técnicas; 1999. p.195-209. 3. Alves AF, Silva MC. Cancro do pulmão no Serviço de Pneumologia do Hospital de Santarém: resultados de 4 anos (2003-2006). HDS InForma. 2008;(22). 4. Sotto-Mayor R. O lugar da quimioterapia na terapêutica do cancro do pulmão. Rev Port Pneumol. 2001;VII:558-94. 5. Barata F. O que o doente deve saber sobre o cancro do pulmão. [acessado em 10 de outubro de 2008]. Disponível em: http://www.sppneumologia.pt/textos/?imc=51n81n 6. Uehara C, Jamnik S, Santoro IL. Câncer de pulmão. Medicina, Ribeirão Preto. 1998;31:266-76. 7. Beckles MA, Spiro SG, Colice GL, et al. Initial evaluation of the patient with lung cancer: symptoms, signs, laboratory tests and paraneoplastic syndromes. Chest. 2003;123(1 Suppl);97S-104S. 8. Kamath A, Chhajed PN. Role of bronchoscopy in the early diagnosis of lung cancer. Indian J Chest Dis Allied Sci. 2006;48:265-9. 9. Carvalho L. A nova classificação de tumores pulmonares - interesse meramente académico? Rev Port Pneumol. 2004;X(1 Supl 1):S9-13. 10. Westeel V. Diagnosis of lung cancer. Rev Prat. 2003;53:727-34. 11. Barcellos MG. Radiologia do câncer de pulmão. J Pneumol. 2002;28:94-9. 12. Cordeiro AJA Robalo. Pneumologia fundamental. Lisboa: Fundação Calouste Gulbenkian; 1995. p.349-73. 13. Herth FJ, Eberhardt R, Ernst A. The future of bronchoscopy in diagnosing, staging and treatment of lung cancer. Respiration. 2006;73:399-409. 14. El-Bayoumi E, Silvestri GA. Bronchoscopy for the diagnosis and staging of lung cancer. Semin Respir Crit Care Med. 2008;29:261-70. 15. Rivera MP, Detterbeck F, Mehta AC; American College of Chest Physicians. Diagnosis of lung cancer: the guidelines. Chest. 2003;123(1 Suppl 1):129S-36S. 16. Gaur DS, Thapliyal NC, Kishore S, et al. Efficacy of broncho-alveolar lavage and bronchial brush cytology in diagnosing lung cancers. J Cytol. 2007;24:73-7. 17. Cook RM, Miller YE. Flexible fiberoptic bronchoscopy in the diagnosis and staging of lung cancer. In: Johnson EB, Johnson HD, editors. Lung cancer. New York, NY: Wiley-Lyss; 1995. p.123-44. 18. Wynants J, Stroobants S, Dooms C, et al. Staging of lung cancer. Radiol Clin North Am. 2007;45:609-25. 19. Queiroga H. Factores de prognóstico "clássicos" no cancro do pulmão. Rev Port Pneumol. 2005;XI(3 Supl 1):S105-11. 20. Sá Vieira V. Cirurgia no doente com cancro do pulmão. [acessado em 10 de outubro de 2008]. Disponível em: http://www.sppneumologia.pt/textos/?imc=51n81n 21. Provencio M, Camps C, Alberola V, et al. Lung cancer and treatment in elderly patients: the Achilles Study. Lung Cancer. 2009;66:103-6. 22. Barros JA, Valladares G, Faria AR, et al. Diagnóstico precoce do câncer de pulmão: o grande desafio. Variáveis epidemiológicas e clínicas, estadiamento e tratamento. J Bras Pneumol. 2006;32:221-7. 23. Novaes FT, Cataneo DC, Ruiz Junior RL, et al. Câncer de pulmão: histologia, estádio, tratamento e sobrevida. J Bras Pneumol. 2008;34:595-60. 24. Westphal FL, Lima LC, Andrade EO, et al. Características de pacientes com câncer de pulmão na cidade de Manaus. J Bras Pneumol. 2009;35:157-63. 25. van Zandwijk N. Aetiology and prevention of lung cancer. Eur Respir Mon. 2001;17:13-33. 26. Stinchcombe TE, Socinski MA. Current treatments for advanced stage non-small cell lung cancer. Proc Am Thorac Soc. 2009;6:233-41. 27. Kerr KM. Pulmonary adenocarcinomas: classification and reporting. Histopathology. 2009;54:12-27. 28. Wang T, Nelson RA, Bogardus A, et al. Five-year lung cancer survival: which advanced stage nonsmall cell lung cancer patients attain long-term survival? Cancer. 2010;116:1518-25. 29. Yasufuku K. Early diagnosis of lung cancer. Clin Chest Med. 2010;31:39-47. 30. Thomas PA. Standards of surgery in lung cancer. Rev Prat. 2009;59:934-8. 31. Simon M, Simon I. Update in bronchoscopic techniques. Pneumologia. 2010;59:53-6. 32. Brandão DS, Haddad R, Marsico GA, et al. Aspectos clínico-patológicos do carcinoma bronquioloalveolar e sobrevida em pacientes no estágio clínico I. J Bras Pneumol. 2010;36:167-74. 33. Herth FJ, Eberhardt R. Flexible bronchoscopy and its role in the staging of non-small cell lung cancer. Clin Chest Med. 2010;31:87-100. 34. Fernandez A, Jatene FB, Zamboni M. Diagnóstico e estadiamento do câncer de pulmão. J Pneumol. 2002;28:219-28. 35. Devbhandari MP, Quennell P, Krysiak P, et al. Implications of a negative bronchoscopy on waiting times to treatment for lung cancer patients: results of a prospective tracking study. Eur J Cardiothorac Surg. 2008;34:479-83. 36. Hansell DM, Boiselle PM, Goldin J, et al. Thoracic imaging. Respirology. 2010;15:393-400. 37. Thiberville L, Salaun M, Lachkar S. New diagnostic tools in lung cancers. Rev Prat. 2009;59:925-31. 38. Jiang F, Todd NW, Qiu Q, et al. Combined genetic analysis of sputum and computed tomography for noninvasive diagnosis of non-small-cell lung cancer. Lung Cancer. 2009;66:58-63. 39. Scagliotti G. Symptoms, signs and staging of lung cancer. Eur Respir Mon. 2001;17:86-119. 40. Madhusudhan KS, Gamanagatti S, Seith A, et al. Pulmonary infections mimicking cancer: report of four cases. Singapore Med J. 2007;48:e327-31. 41. Sawai T, Soda H, Kohno S. Mycobacterium intracellulare pulmonary infection which co-existed and mimicked lung cancer. Intern Med. 2008;47:459-62. 1. Licentiate in Radiology, Radiologic Technologist, Escola Superior de Tecnologia da Saúde de Coimbra (ESTeSC), Coimbra, Portugal 2. Master, Professor at Escola Superior de Tecnologia da Saúde de Coimbra (ESTeSC), Coimbra, Portugal Study developed at Hospital Distrital da Figueira da Foz (HDFF), Escola Superior de Tecnologia da Saúde de Coimbra (ESTeSC), Coimbra, Portugal Mailing address: António Saraiva Escola Superior de Tecnologia da Saúde de Coimbra (ESTeSC) Rua 5 de Outubro. S. Martinho do Bispo, Apartado 7006 3046-854 Coimbra, Portugal E-mail: asaraiva@estescoimbra.pt Received November 6, 2009 Accepted after revision July 16, 2010 |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554