Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 4 - July / Aug. of 2010
Vol. 43 nº 4 - July / Aug. of 2010
|
ORIGINAL ARTICLE
|
|
Reproducibility of fetal limbs volume by three-dimensional ultrasonography utilizing the XI VOCAL method |
|
|
Autho(rs): Rafael Oliveira Cavalcante1, Edward Araujo Júnior2, Luciano Marcondes Machado Nardozza3, Liliam Cristine Rolo4, Antonio Fernandes Moron5 |
|
|
Keywords: Reproducibility; Fetal limbs volume; Three-dimensional ultrasonography; XI VOCAL. |
|
|
Abstract: INTRODUCTION
Fetal growth disorders are important causes of increased perinatal morbidity and mortality. Poor neonatal outcomes may result from macrosomia (birth trauma) and intrauterine growth restriction (asphyxia)(1,2). The fetal limbs volume has been associated with fetal growth and nutritional status(3). Initially, fetal thigh volume (TVol) and upper arm volume (AVol) were indirectly estimated by means of two-dimensional ultrasonography (2D US). However, 2D US cannot provide an accurate measurement of fetal limbs volume. Most of the studies on the volumetric evaluation of fetal limbs by 2D US calculate the volume by means of a cross sectional area obtained from a single section plane, being subject to errors, considering that the section may not be the most appropriate one(4,5). In another study, the TVol and AVol were calculated assuming that the limbs were cylindrical(3), which obviously does not correspond to reality. The advent of three-dimensional ultrasonography (3D US) has allowed a more accurate volumetric evaluation than 2D US, as it allows the outlining of the outer surface of the object, which is particularly important for irregularly shaped structures6). Considering that TVol and AVol are well established parameters as markers for fetal growth and nutrition, several studies have utilized these limbs volume as predictors for birth weight, obtaining more reliable results than those from the traditional formulas utilized by 2D US(7-9). In all of such studies, the multiplanar or planimetric method was utilized. This technique consists of delimitating multiple sequential planes along an axis and, at the end of the course along the axis, the equipment performs the sum of the areas and the volume is automatically calculated(6). The main inconvenience of this technique is the relatively long time required for the volumetric calculation of fetal limb volumes(7,8). Recently a new volumetric technique called eXtended Imaging Virtual Organ Computer-aided AnaLysis (XI VOCAL) became available as part of the Three-dimensional eXtended Imaging (3D XI - Medison; Seoul, Korea) software. Such technique consists of the delimitation of areas of sequential adjacent planes displayed on the apparatus screen (multislice view), and at the end of the process the equipment sums up the areas, automatically providing the volume as well as the distance between initial and end plane and slices thickness(10). Two studies have evaluated the application of such technique in vivo, one of them in the evaluation of fetal volumes between the 11th and 14th gestational weeks(11), and the other in the measurement of the gestational sac volume between the 7th and 11th gestational weeks(12), however, no description for the fetal limbs volume is found in the literature. The objective of the present study is to evaluate the interobserver reproducibility of the measurements of fetal upper arm and thigh volume by means of 3D US, utilizing the XI VOCAL method. MATERIALS AND METHODS A prospective observational study was developed with 43 healthy pregnant women between the 20th and 37th gestational weeks in order to assess the reproducibility of 3D US in the fetal limbs volume evaluation by utilizing the XI VOCAL method. The study was developed at the Unit of Three-Dimensional Ultrasonography, Department of Obstetrics at Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil, with randomly selected patients. The study was approved by the Committee for Ethics in Research of Unifesp, under number 4843/09, and all the participating patients signed a Term of Free and Informed Consent. Inclusion criteria were the following: (1) singleton gestation with live fetus and (2) gestational age determined by the last menstruation date, in women with regular menstrual cycles, and confirmed by ultrasonography performed in the first trimester, utilizing as a parameter the crown-rump length (CRL). Exclusion criteria were the following: (1) fetuses with structural abnormalities detected at ultrasonography; (2) pregnant women with chronic diseases that might affect the fetal growth; (3) alterations in the volume of amniotic fluid, with amniotic fluid index (AFI) below the 5th or above the 95th percentile for gestational age, according to the table proposed by Moore & Cayle(13); (4) fetuses with weight prediction below the 10th or above the 90th percentile, according to the table proposed by Hadlock et al.(14). All the sonographic studies were performed with an Accuvix XQ (Medison; Seoul, Korea) apparatus, equipped with an automatic scan multi-frequency convex transducer (C3-7ED). All the studies were performed by a single observer, with two-year experience in obstetric 3D US. Initially a 2D real time evaluation was performed in order to determine biometry, morphology, amniotic fluid volume quantification and fetal weight prediction. Standard planes for the measurement of the humerus and the femur length were utilized for the acquisition of limb volumes, selecting the limb that was closest to the transducer (anterior wall of the uterus), considering that there is no statistically significant difference between the left and the right limbs(7,8). The volume acquisition was performed during absolute fetal rest and by requesting the patient to hold the breath for few seconds. The following settings were standardized: aperture angle ranging from 50º to 70º depending on gestational age, normal velocity mode, high definition and harmonic mode. The scanning box was adjusted in such a way to comprise the whole fetal limb (region of interest - ROI), and subsequently the automatic 3D scan was performed. Two volumes of each fetal limb, upper arm or thigh, were acquired for each patient, with the one with best quality being selected for volumetric measurement. After the volume acquisition, the image was presented in the multiplanar mode (axial, sagittal and coronal). The sagittal plane was selected as a reference. For the volumetric calculation, the XI VOCAL method included in the 3D XI software (Medison; Seoul, Korea) was utilized, selecting the proximal and distal epiphyses of the limb as the initial and end planes, respectively. The arbitrary option for manual delimitation of 10 areas was made, obtaining a diagram of cross sections of the fetal limb (multislice view - Medison; Seoul, Korea), that simultaneously showed a sequence of images in parallel planes. After the manual outlining of the external surface of all selected planes, the equipment automatically supplied the limb's volume, as well as the respective distance between the initial and last planes and slices thickness (Figure 1). 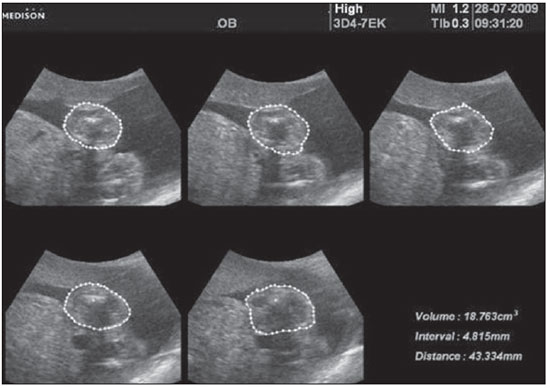 Figure 1. Utilization of the XI VOCAL method with manual delineation of 10 consecutive planes of the fetal thigh (axial plane), represented on this image by 5 planes. Notice on the right lower corner, the final volume, besides the distances between the initial and end-planes and between intermediate planes. The volumetric analyses were performed off line by means of the software SonoView-Pro version 1.03 (Medison; Seoul, Korea). The main observer performed one measurement of the upper arm and thigh volumes of 43 fetuses. The same volumes were blindly measured by a second observer. The data were recorded on an Excel 2003 worksheet (Microsoft Corp.; Redmond, WA, USA) and were analyzed by the Statistical Package for the Social Sciences (SPSS) version 15.0 for Windows (SPSS Int.; Chicago, IL, USA). The reproducibility, which consists in the capacity of a test to produce the same result between different observers (interobserver variability), was calculated by utilizing the paired Student's t test (p), the intraclass correlation coefficient (ICC) and Bland Altman plots(15). The ICC < 0.40 is considered as being poor, satisfactory between 0.40 and 0.75 and excellent when ICC > 0.75(16). The Bland-Altman plots analyze the mean values of the measurements performed by one or two observers, against the difference of their measurements with a confidence interval of 95% and 1.96 standard deviation from the mean. In all the analyses, the significance level (p) 0.05 was utilized. RESULTS Forty three healthy pregnant women were evaluated between the 20th and 37th gestational weeks. The mean maternal age was 29 ± 5.36 years (standard deviation), while the number of gestations was 2 ± 1.54 gestations. A high interobserver reproducibility was observed, both for the upper arm and fetal thigh volumes. For the upper arm volume, the obtained ICC was 0.996 (CI 95%: 0.992; 0.998). By utilizing the Bland-Altman plot for the upper arm volume (Figure 2), one observed that most of the points representing the difference between the measurements are within the confidence interval (only two points are out of the confidence interval, corresponding to 4.65% of the sample), which demonstrates that there is no statistically significant difference, with p < 0.05. The mean difference was 0.13 ± 1.29% (95% agreement limits: -2.54; +2.54%). For the thigh volume, the obtained ICC was 0.997 (CI 95%: 0.995; 0.999). On the Bland-Altman plot for thigh volume (Figure 3), one observed that all points representing the differences between the measurements are within the confidence interval (only one point is out of the standard deviation, corresponding to 2.3% of the sample) which demonstrates that there is no statistically significant difference, with p < 0.05. The mean difference was 0.24 ± 7.60%, with (95% agreement limits: -7.6; +7.6%). 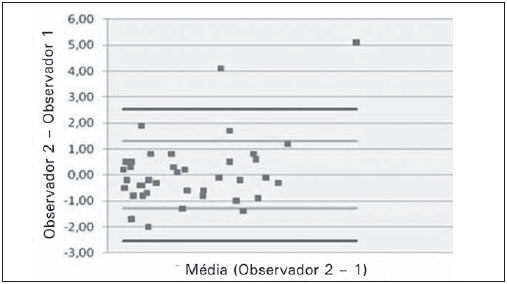 Figure 2. Difference of the measurements performed by two observers (observer 1 and observer 2) plotted against the difference of their means for the fetal upper arm volume by the XI VOCAL method. 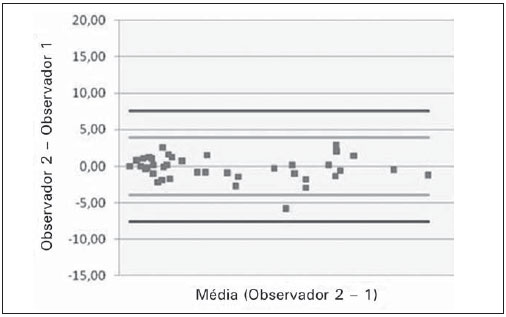 Figure 3. Difference of measurements performed by two observers (observer 1 and observer 2) plotted against the difference of their means for the fetal thigh volume by the XI VOCAL method. DISCUSSION In the present study, the authors demonstrated a high interobserver reproducibility of the measurements of fetal upper arms and thighs by means of 3D US utilizing the XI VOCAL method. The XI Vocal method is a recent technique for volumetric calculation available as a resource of the 3D XI (Medison; Seoul, Korea) software. Such technique consists in delimitating areas in sequential adjacent planes (multislice view)(10). The observer determines an initial- and an end-plane, besides the number of planes between these limits (5, 10, 15 and 20). The type of delineation can be manual, cystic or general. For each plane delimitation an area is determined and, after the delimitation of all planes, the equipment automatically provides the volume, besides the interval between the intermediate planes and the distance between initial and end-planes. At the end of the delimitation of the last plane the software allows the edition of all previous planes in order to make corrections that may be necessary. Two studies have evaluated the application in vivo of this new software(11,12). In the first one, the volumes of 30 fetuses between the 11th and 14th gestational weeks were compared by the multiplanar, VOCAL and XI VOCAL, with good intra and interobserver reproducibility being observed for this technique, with ICC > 0.9 for 10, 15 and 20 planes(11). In the other study, gestational sac volumes were compared by means of the multiplanar, VOCAL and XI VOCAL methods between 7 and 11 gestational weeks with strong correlation being observed among them (XI VOCAL vs. multiplanar: ICC = 0.995; XI VOCAL vs. VOCAL: ICC = 0.998; and multiplanar vs. VOCAL: ICC=0.995)(12). Studies have demonstrated that upper arm and thigh volumes are important parameters in the prediction of intrauterine growth restriction(17-19). Additionally, the determination of the fractional limb volume, the central portion of the limb that contains the greatest amount of soft tissue, has been shown to be an effective parameter in the early detection of fetal growth disorder(20,21). However, few studies have been proposed to evaluate the reproducibility of the measurement of fetal limbs in such a way to validate the clinical use of this relevant fetal growth parameter(22,23). In the study developed by Chang et al.(22), the authors have determined reference values for the upper arm volume in 204 fetuses between 20 and 40 gestational weeks and, additionally, they calculated the intraobserver reproducibility by repeating the measurements with 21 fetuses, obtaining a high determination coefficient (R2 = 0.9958). One should mention the following limitations in this study: the absence of data on interobserver variability, the small number of evaluated cases and the non utilization of appropriate tests for reproducibility studies (ICC and Bland-Altman plots(15,16)). In the present study, which evaluated 43 fetuses, the ICC for the upper arm volume was 0.996 and the mean difference was 0.13%, while the ICC for the thigh volume was 0.997 and the mean difference was 0.24%. In a study evaluating the fractional upper arm and thigh volumes, Lee et al.(23) have obtained the value of - 1.9% for the mean difference of interobserver reproducibility of the fractional upper arm volume, while for the fractional thigh volume the obtained value was - 2.0%, results similar to those obtained in the present study, in which the volume of the whole limb was evaluated. In summary, the present study demonstrated the high reproducibility of the XI VOCAL method in the measurement of fetal limbs volume, making its use possible in the clinical practice as a new parameter for the evaluation of the fetal nutritional status. Such technique presents as advantages the swiftness in calculation, differently from the multiplanar method, besides the capability of modifications in the contours. As a limitation, the restricted availability of the method should be mentioned, as it is an exclusive resource in Medison Accuvix XQ, V 10 and V20 apparatuses. CONCLUSION The fetal upper arm and thigh volumes calculated by 3D US utilizing the XI VOCAL method presented a high interobserver reproducibility between 20 and 37 gestational weeks. REFERENCES 1. Roth S, Chang TC, Robson S, et al. The neurodevelopmental outcome of term infants with different intrauterine growth characteristics. Early Hum Dev. 1999;55:39-50. 2. Dashe JS, McIntire DD, Lucas MJ, et al. Effects of symmetric and asymmetric fetal growth on pregnancy outcomes. Obstet Gynecol. 2000;96:321-7. 3. Jeanty P, Romero R, Hobbins JC. Fetal limb volume: a new parameter to assess fetal growth and nutrition. J Ultrasound Med. 1985;4:273-82. 4. Warda A, Deter RL, Duncan G, et al. Evaluation of fetal thigh circumference measurements: a comparative ultrasound and anatomical study. J Clin Ultrasound. 1986;14:99-103. 5. Vintzileos AM, Campbell WA, Rodis JF, et al. Fetal weight estimation formulas with head, abdominal, femur and thigh circumference measurements. Am J Obstet Gynecol. 1987;157:410-4. 6. Riccabona M, Nelson TR, Pretorius DH. Three-dimensional ultrasound: accuracy of distance and volume measurements. Ultrasound Obstet Gynecol. 1996;7:429-34. 7. Chang FM, Liang RI, Ko HC, et al. Three-dimensional ultrasound-assessed fetal thigh volumetry in predicting birth weight. Obstet Gynecol. 1997;90:331-9. 8. Liang RI, Chang FM, Yao BL, et al. Predicting birth weight by fetal upper-arm volume with use of three-dimensional ultrasonography. Am J Obstet Gynecol. 1997;177:632-8. 9. Song TB, Moore TR, Lee JY, et al. Fetal weight prediction by thigh volume measurement with three-dimensional ultrasonography. Obstet Gynecol. 2000;96:157-61. 10. Guimarães Filho HA, da Costa LL, Araujo Júnior E, et al. XI VOCAL (eXtended Imaging VOCAL): a new modality for three-dimensional sonographic volume measurement. Arch Gynecol Obstet. 2007;276:95-7. 11. Cheong KB, Leung KY, Chan HY, et al. Comparison of inter- and intraobserver agreement between three types of fetal volume measurement technique (XI VOCAL, VOCAL and multiplanar). Ultrasound Obstet Gynecol. 2009;33:287-94. 12. Nardozza LM, Rolo LC, Araujo Júnior E, et al. Comparison of gestational sac volume by 3D-sonography using planimetric, virtual organ computer-aided analysis and extended imaging virtual organ computer-aided analysis methods between 7 and 11 weeks of pregnancy. Acta Obstet Gynecol Scand. 2010;89:328-34. 13. Moore TR, Cayle JE. The amniotic fluid index in normal human pregnancy. Am J Obstet Gynecol. 1990;162:1168-73. 14. Hadlock FP, Harrist RB, Carpenter RJ, et al. Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology. 1984;150:535-40. 15. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307-10. 16. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420-8. 17. Chang CH, Yu CH, Ko HC, et al. The efficacy assessment of thigh volume in predicting intrauterine fetal growth restriction by three-dimensional ultrasound. Ultrasound Med Biol. 2005; 31:883-7. 18. Chang CH, Yu CH, Ko HC, et al. Fetal upper arm volume in predicting intrauterine growth restriction: a three-dimensional ultrasound study. Ultrasound Med Biol. 2005;31:1435-9. 19. Araujo Júnior E, Vieira MF, Nardozza LM, et al. Ultra-som tridimensional na avaliação do volume de membros fetais. Radiol Bras. 2007;40:349-53. 20. Lee W, Deter RL, McNie B, et al. Individualized growth assessment of fetal soft tissue using fractional thigh volume. Ultrasound Obstet Gynecol. 2004;24:766-74. 21. Lee W, Deter RL, McNie B, et al. The fetal arm: individualized growth assessment in normal pregnancies. J Ultrasound Med. 2005;24:817-28. 22. Chang CH, Yu CH, Chang FM, et al. Assessment of normal fetal upper arm volume by three-dimensional ultrasound. Ultrasound Med Biol. 2002;28:859-63. 23. Lee W, Balasubramaniam M, Deter RL, et al. Fractional limb volume - a soft tissue parameter of fetal body composition: validation, technical considerations and normal ranges during pregnancy. Ultrasound Obstet Gynecol. 2009;33:427-40. 1. Fellow Master degree, MD, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil 2. Post Doctor, Affiliate Professor, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil 3. Private Docent, Associate Professor, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil 4. Master, MD, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil 5. Private Docent, Titular Professor, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil Study developed in the Unit of Three-Dimensional Ultrasonography, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil Mailing address: Dr. Edward Araujo Júnior Departamento de Obstetrícia - Universidade Federal de São Paulo (Unifesp) Rua Napoleão de Barros, 875, Vila Clementino 04024-002. São Paulo, SP, Brazil E-mail: araujojred@terra.com.br Received April 6, 2010 Accepted after revision May 14, 2010 |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554