Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 4 - July / Aug. of 2007
Vol. 40 nº 4 - July / Aug. of 2007
|
ORIGINAL ARTICLE
|
|
Manikin-type training simulator model for transpedicular puncture in percutaneous vertebroplasty |
|
|
Autho(rs): Nitamar Abdala, Ricardo Abdala da Silva Oliveira, João de Deus da Costa Alves Junior, Tulio Spinola |
|
|
Keywords: Spine, Puncture, Learning, Manikin, Vertebroplasty |
|
|
Abstract:
IPhD, Affiliated Professor, Departamento de Diagnóstico por Imagem da Universidade Federal de São Paulo-Escola Paulista de Medicina (Unifesp-EPM), São Paulo, SP, Brazil
INTRODUCTION Percutaneous vertebroplasty is a radiological procedureinvolving puncture and injection of acrylic cement into avertebral body(1). This procedure is indicatedin cases of fractures resulting from osteoporosis, malignanthemangiomas and metastases(1,2). Currentstudies report analgesia(3), improvement inmovements amplitude(3,4) and strengthening ofthe bone matrix(1), after the procedure. Percutaneous vertebroplasty is included in the therapeuticarsenal for several specialties among which interventionalradiology(5). Aiming at medical professionals qualifying,workshops(6,7) provide them with theoreticalknowledge and practical training. For the purposes of thisteaching model, simulator models constitute invaluable tools toimprove the medical trainees skills and confidence in complex andrisky procedures, to keep the abilities acquired throughsimulated exercises even when therapeutic procedures are notbeing performed, and, finally, to provide a researchfield(8). In the present study, the authors propose the development andevaluation of a manikin-type training model for transpedicularpuncture in percutaneous vertebroplasty.
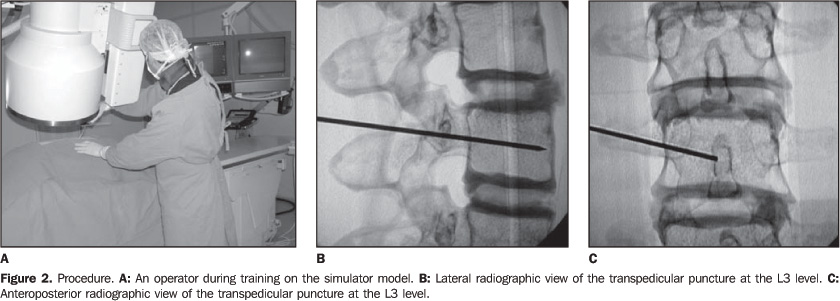
MATERIALS AND METHODS Simulator Vertebral segments were developed with molds of human lumbar vertebrae filled with a methacrylate and plaster (Figure 1A). The pulpy nucleus in the core of each vertebral body was simulated by a piece of sponge soaked with a methacrylate solution. Then, five of these vertebrae were grouped, constituting the lumbar segment of a spinal column. Disc spaces were filled with fragments of sponge soaked with a solution of polydimethylsiloxane and silica, imitating intervertebral discs (Figure 1B). The necessary vertebral bodies alignment was kept by means ofstrips of ethylene vinyl acetate inserted between spinalprocesses, and articular facets were stuck together with a pastemade of polydimethylsiloxane and silica. The next step consisted of reproducing a human trunk, with a commercial plastic manikin called shell, with a wide lumbardorsal opening allowing the access to the inside of the shell. A wooden support was fixed into the shell with pressure screws and nuts. Two 2 cm-thick strips of ethylene vinyl acetate with 30 cm in length and height ranging between 4 cm at the middle third and 5 cm at the ends were fixed on the support. This structure allowed a stable positioning of the spinal column in a lordotic position on the wooden support (Figure 1C). Finally, the access to the inside of the shell was limited by a coat of ethylene vinyl acetate, fixed to the border of the shell (Figure 1D), representing the skin. Procedure Each trainee should perform 30 transpedicular punctures in three series of ten punctures each, with one-week interval between series. The procedure was performed under fluoroscopy in a Philips Integris V5000 angiograph, with a Gallini®13-gauge needle for percutaneous vertebroplasty, in compliance with the technique described by Cotten et al.(1) (Figure 2A). Any construction failure detected during the procedures would determine the exclusion of such procedure for the effects of the learning curve results. At the end of each training session, a methacrylate solutionwas applied to occlude the puncture pathway, allowing a newutilization of the vertebra model, up to threereutilizations. The procedures were recorded on CDs and radiographic films (Figures 2B and 2C). Model evaluation The training model was evaluated by six trainees inneuroradiology familiarized with the method, but withoutexperience in vertebroplasty. All of them answered aquestionnaire about: the possibility, or not, of visualizing thespinal column within the closed shell, without radiological aid;the possibility, or not, of identifying and individualizing thecortical and spongiosa layers at fluoroscopy and radiography;whether the respondents could perceive the differences betweennew and reutilized components; and finally, they were askedsuggestions to improve the training model.
RESULTS One hundred and seventy-two of the 180 procedures performedwere considered as appropriate. Eight procedures were excludedbecause of a posterior displacement of the vertebra during theprocedure due to a failure in the attachment of the vertebra tothe shell structure. Similarity data forms were filled in by all of the traineesfollowing the procedures. All of them were unanimous as regardsthe non-visualization of the spinal column within the closedshell without radiological aid. All of them confirmed that theyhad observed a great anatomical similarity, a good visualizationof the pedicle and cortical and spongiosa layers at fluoroscopyand radiography, as well as a clear tactile perception of theselayers during the needle insertion. No significant difference wasobserved between new and restored components during theprocedures. As regards suggestions, three of the appraisers mentioned thelow weight of the simulator model, allowing mobility of the trunkduring the procedures. Four appraisers highlighted the necessityof intermediate planes simulating the musculature, just like invivo procedures.
DISCUSSION According to Kneebone & ApSimon(9), theeffectiveness of a learning model based only on observation isquestionable because it fails to stimulate a deep involvement ofthe trainee so the training is not effective. Therefore, skillsacquisition, especially in the fields of surgery andinterventional procedures, demands a sustained practice. On theother hand, the utilization of patients for practice andexperience acquisition by trainees during their initial phase ofeducation is unacceptable because of medical/ethical/legalconcerns. So, the utilization of a simulator model constitutes anoption for training, acquisition and evaluation of skills bymeans of a repeated safe practice(10). The utilization of animal models has the disadvantage of highcost and poor reproducibility, besides difficulties of ethicalnature(9,11). Another difficulty would be theanatomical issue since the variability of animal models couldrepresent a disadvantage in the definition of a paradigm, aspointed out by Gailloud et al.(11), in a studyon the development of in vitro models for dural fistulas. As regards the development of in vitro models, Bartynski etal.(12) and Kerber et al.(13)have shared the interest in alternative models, and, for thepurposes of training and research, they have develop a model ofarteriovenous malformation for simulating therapeuticembolization. In this context, the proposition of the presentstudy is compatible with the idea of developing a non-animalmodel for guaranteeing the acquisition by interventionalprofessionals of technical qualification previously to theperformance of percutaneous vertebroplasty in patients. According to Kneebone(10), in a study aboutmedical education, simulators may be based on physical models, onthe virtual reality, and on the so called hybrid models. Themodel described in the present study can be classified as aphysical simulator model with a great technological appealconsidering the wide range of materials involved in itsconstruction. On the other hand, these training models arelimited just to a body segment, and, for being inanimate, they donot allow a great model/operatorinteraction(10). Panjabi(14) classifies the cervical spinemodels for biomechanical research as physical models, emphasizingits simplicity, low cost and low variability, considerationsequally compatible with the simulator model proposed by thepresent study. On the other hand, this author affirms thatphysical models of the spinal column give little importance tothe osseous anatomy and physical properties of adjacent softtissues, and are principally utilized for surgicalinstrumentation testing. As regards anatomy, the results of thepresent study diverge from the Panjabi'sassertion(14), since, despite the littleconcern with paravertebral structures, all of the appraisers(100% positive answers) observed a great anatomical similarity ofthe model with an actual patient, probably because themanufacture of this model was based on molds for componentsreproduction, as described by Gailloud etal.(11), and also because of vertebral layersstratification allowing a great visual similarity at fluoroscopyand tactile perception during the procedure. Another aspect to be discussed is the reutilization ofcomponents. The restoration resulted in a satisfactory occlusionof the puncture site, and, due to the presence of the coat ofethylene vinyl acetate, the operator could not directly visualizethe restored areas, not even by fluoroscopy. The reason probablyis that the spongeous material of the internal layer refills thepuncture pathway as soon as needle is withdrawn, so reducing thetraining costs. According to suggestions from three appraisers, it isunderstood that some features of this simulator should be changedto increase the model similarity with the human body. Among them,the simulator weight should be increased to avoid mobility of thetrunk during the procedures, and intermediate planes should becreated to provide a tactile perception, particularly of themusculature, during the insertion of the needle through theseplanes.
CONCLUSION The training simulator model described in the present studypresents characteristics of similarity with in vivoprocedure and should be considered as a potential tool formedical training in transpedicular puncture. The mentionedsuggestions corroborate the aim at searching for materialimprovement and increase in realism.
REFERENCES 1. Cotten A, Boutry N, Cortet B, et al. Percutaneous vertebroplasty: state of the art. RadioGraphics 1998;18:311–320. [ ] 2. Lin DDM, Gailloud P, Murphy K. Percutaneous vertebroplasty in benign and malignant disease. Neurosurg Quart 2001;11:290–301. [ ] 3. Levine SA, Perin LA, Hayes D, Hayes WS. An evidence-based evaluation of percutaneous vertebroplasty. Manag Care2000;9:56–63. [ ] 4. Evans AJ, Jensen ME, Kip KE, et al. Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty – retrospective report of 245 cases. Radiology 2003; 226:366–372. [ ] 5. Strother CM. Interventional neuroradiology. AJNR Am J Neuroradiol 2000;21:19–24. [ ] 6. Faculty will discuss percutaneous vertebroplasty versus kyphoplasty as well as current standards and research. The afternoon hands-on workshop will highlight [on line]. [cited 2004 Sept 24]. Available from: https://www.eddesign.com/May/Treating0502.html [ ] 7. Minimally Invasive Spinal Surgery Workshop. Vertebroplasty new technique on percutaneous discectomy [on line]. Course Chairman: Dr. Kwai Fung. Prince of Wales Hospital. [cited 2004 Sept 24]. Available from: http://www.olc-cuhk.org/eng/calendar/program/20040805MISS.asp [ ] 8. Schijven MP, Jakimowicz J. The learning curve on the Xitact LS 500 laparoscopy simulator: profiles of performance. Surg Endosc 2004;18:121–127. [ ] 9. Kneebone R, ApSimon D. Surgical skills training: simulation and multimedia combined. Med Educ 2001;35:909–915. [ ] 10. Kneebone R. Simulation in surgical training: educational issues and practical implications. Med Educ 2003;37:267–277. [ ] 11. Gailloud P, Muster M, Piotin M, et al. In vitro models of intracranial arteriovenous fistulas for the evaluation of new endovascular treatment materials. AJNR Am J Neuroradiol 1999;20:291–295. [ ] 12. Bartynski WS, O'Reilly GV, Forrest MD. High-flow-rate arteriovenous malformation model for simulated therapeutic embolization. Radiology 1988;167:419–421. [ ] 13. Kerber CW, Hecht ST, Knox K. Arteriovenous malformation model for training and research. AJNR Am J Neuroradiol 1997;18:1229–1232. [ ] 14. Panjabi MM. Cervical spine models for biomechanical research. Spine 1998;23:2684–2700. [ ]
Received September 25, 2006. Accepted after revision November 30, 2006.
* Study developed at UMDI Diagnósticos, Mogi das Cruzes, SP, and Departamento de Diagnóstico por Imagem da Universidade Federal de São Paulo-Escola Paulista de Medicina (Unifesp-EPM), São Paulo, SP, Brazil. |
|

{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554