Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 3 - May / June of 2007
Vol. 40 nº 3 - May / June of 2007
|
CASE REPORT
|
|
Embolism caused by metallic mercury: a case report |
|
|
Autho(rs): João Paulo Kawaoka Matushita, Roberto Márcio A. Peixoto, Hilton Muniz Leão Filho, Guilherme Carvalho Missiaggia, Ricardo Saraiva Dias, Wilson Campos Tavares Junior, Cristina Sebastião Matushita, José Nelson Mendes Vieira |
|
|
Keywords: Embolism, Mercury, Radiology, Computed tomography |
|
|
Abstract:
IPhD, Associate Professor at Faculdade de Medicina da Universidade Federal de Minas Gerais (UFMG), Full Professor of Radiology and Imaging Diagnosis, Course of Physiotherapy at Faculdade Biológicas da Saúde do Centro Universitário Newton Paiva, Belo Horizonte, MG, Brazil
INTRODUCTION Reports on metallic mercury injection are unusual in the literature, and embolism caused by these metallic particles is rare. Most frequent causes are intravenous injections defined as suicide attempts(1,2) or a complication resulting from drugs abuse(3). Injection of mercury by accident may occur because of injuries from a broken thermometer(4,5). Subcutaneous administration(6,7) or vascular migration following injection(2,3,8) may result in granulomas and abscesses in the site. Systemic signs of toxicity by mercury are not found immediately; however, four cases have been found in the literature with systemic manifestation after a subcutaneous injection(9,10).
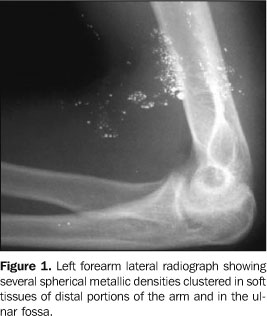
CASE REPORT Male, 29-year-old patient, born in Divinópolis, MG, Brazil, who, in January/1988, with 16 years of age, tried to suicide with a subcutaneous auto-injection of 2 ml metallic mercury into his left forearm. Eight hours post-injection, he presented an increased tenderness in the region of the injection, with "tugging" and loss of coordination in the trunk and in the correspondent upper limb lasting for about three days. He sought medical assistance in the following day, by the doctor did not believe him and no laboratory test or study was requested. Some weeks later, the patient presented with an inflammatory foreign-body-type reaction at the site of the injection which had to be surgically drained for three times, eliminating a solid, silvery material resembling sand grains. The patient developed anorexia with a 10 kg weight loss in few weeks. Clinically, he complained of excessive sudoresis, somnolence, and metallic taste in the mouth. As regards family antecedents, the patient reported suicidal ideas after his parents´ separation, when he was eight years old. On physical/neurological examination, the patient presented intentional tremor, with upper spastic paraparesis at left, shuffling walk and hyperreflexia of lower limbs. On clinical examination of the left arm, firm, tumor-like lesions covered by erythemato-violaceous and smooth skin could be observed. One of these lesions presented an elastic consistency, with fluctuation in the cubital fossa. Among the lesions, there was a 5 cm-long and 1 cm-wide fibrotic cord. His left upper limb extension was impaired. Radiological studies demonstrated: left forearm radiograph – multiple spheres with a metallic density subcutaneously clustered in the olecranal fossa, and other, sparse along the veins of the correspondent arm (Figure 1); chest radiographs – several spheres with a metallic density, bilaterally sparse throughout the pulmonary parenchyma and heart shadow (Figure 2); plain abdominal radiograph – some spherical structures with a metallic density in the liver, spleen and abdominal vessels (Figure 3); brain computed tomography (without infusion of hydrosoluble iodinated contrast agent) – small sphere with a metallic density on the left cerebellar hemisphere (Figure 4).
Laboratory tests showed normal levels of urea, creatinine, bilirubin as well as normal hemogram values. Measurements of 24-hour urinary mercury excretion showed the following values: May/1990, 81µg/l; July/1990, 71µg/l; February/1993, 340µg/l; August/2000, 60.7 µg/l (reference value: up to 5 µg/l; biological tolerance limit: 50 µg/l). Electroneuromiography performed in July/2001 was normal. On July 13, 1989, the patient was successfully submitted to surgical excision of the lesion in the left upper limb, with skin graft. The anatomopathological report on the surgical specimen described: macroscopy – irregular fragment of fibrotic tissue measuring 10 cm × 4,6 cm × 4 cm, with areas covered by ulcerated skin, presence of fragments of fibrotic tissue in pellets of inorganic mercury; microscopy – dermis in granulation tissue and intense histiocytic reaction, with microabscesses forming granulomas; blackened, round structures varying in size, lymph nodes presenting follicles with enlarged centers and signs of phagocytosis. Diagnosis: Chronic granulomatous inflammation secondary to foreign body. Lymph nodes in reactional status. Sinusal histiocytosis.
DISCUSSION Subcutaneous deposition of metallic mercury with formation of granulomas occurs because of leakage during the attempt of intravascular injection(3,11–13). Accidents may occur with arterial pressure monitors with a liquid mercury manometer connected to an intra-arterial needle. Radiologically, mercury emboli present as small metallic densities in soft tissues of extremities, distal to the site of the manometer needle insertion(14). Venous embolization caused by mercury results from accidents, suicide attempts(1,2) and thermometers break(4,5). Radiological findings in patients with metallic mercury emboli in the vascular system identify multiple small, spherical metallic densities in the drainage pathways at the site of insertion, and also in one or both lungs. Probably, the most difficult differential radiological diagnosis would be between mercury emboli through the pulmonary artery which may occur by venous way, and intrabronchial mercury, which may be aspirated in case of a thermometer break inside the oral cavity. Identification of mercury inside abdominal vessels, in the right ventricle apex, or in subcutaneous tissue of extremities suggests the arterial pathway as route of entry, and identification of intraintestinal mercury suggests the metal ingestion.
REFERENCES 1.Johnson HR, Koumides O. Unusual case of mercury poisoning. Br Med J 1967;1:340–341. [ ] 2.Roden R, Fraser-Moodie A. Self-injection with mercury. Injury 1993;24:191–192. [ ] 3.Netscher DT, Friedland JA, Guzewicz RM. Mercury poisoning from intravenous injection: treatment by granuloma resection. Ann Plast Surg 1991;26:592–596. [ ] 4.Rachman R. Soft-tissue injury by mercury from a broken thermometer. A case report and review of the literature. Am J Clin Pathol 1974;61:296–300. [ ] 5.Tanner DC, Branch M, Schreiner RD, Morgan HJ. Subcutaneous deposition of elemental mercury. J Tenn Med Assoc 1988;81:698–699. [ ] 6.Hill DM. Self-administration of mercury by subcutaneous injection. Br Med J 1967;1:342–343. [ ] 7.Gebauer K, Connor B. Cutaneous mercury granuloma. Australas J Dermatol 1991;32:129–132. [ ] 8.Hannigan BG. Self-administration of metallic mercury by intravenous injection. Br Med J 1978; 2:933. [ ] 9.Kumar A, Jain R, Sawhney S, Goel AK, Chattopadhyay K. Intravenous administration of metallic mercury with homicidal intent. J Assoc Physicians India 1992;40:640–641. [ ] 10.Schulz E, Beskind H. Systemic deposition of metallic mercury. J Pediatr 1960;57:733–737. [ ] 11.Oliver RM, Thomas MR, Cornaby AJ, Neville E. Mercury pulmonary emboli following intravenous self-injection. Br J Dis Chest 1987;81:76–79. [ ] 12.Berger RL, Madoff IM, Ryan TJ. Mercury embolization during arterial pressure monitoring. J Thorac Cardiovasc Surg 1967;53:285–287. [ ] 13.Esau P. Flooding of pulmonary circulation with mercury. Deutsche Ztschr f. Chir 1924;188:221–233. [ ] 14.Ekert F. Multiple mercury deposition roentgenogram of heart, lungs, and spleen in case of milliary tuberculosis. Fortschr a. d. Geb d. Röntgenstrahlen 1950;72:470–473. [ ]
Received April 12, 2005.
* Study developed in the Department of Radiology and Imaging Diagnosis of Hospital das Clínicas, Faculdade de Medicina da Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil. |
|



{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554