Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 3 - May / June of 2007
Vol. 40 nº 3 - May / June of 2007
|
RADIOLOGY UPDATE
|
|
Three-dimensional ultrasonography in the evaluation of the fetal cerebellum |
|
|
Autho(rs): Edward Araujo Júnior, Hélio Antonio Guimarães Filho, Cláudio Rodrigues Pires, Luciano Marcondes Machado Nardozza, Antonio Fernandes Moron |
|
|
Keywords: Fetus, Cerebellum, Volume of organs, Prenatal diagnosis, Three-dimensional ultrasound |
|
|
Abstract:
INTRODUCTION The embryonic development of the cerebellum starts in the fifth week of gestation as a protuberance covering the floor of the fourth ventricle(1). The cerebellum, an organ of the infratentorial nervous system, originates from the dorsal portion of the metencephalon, and is situated dorsally to the bulb and pons, delimiting part of the fourth ventricle. In the middle portion of the cerebellum, the cerebellar vermis is distinguishable, connecting two great lateral masses — the cerebellar hemispheres(2). Early in the end of the first quarter of gestation, the cerebellum can be identified by means of ultrasound(3). However, the early diagnosis of posterior fossa abnormalities should be avoided before the 18th week of gestation, since the cerebellar vermis is not completely developed at this gestational age (GA)(4). Alterations in the sonographic aspect of the cerebellum (shape and echogenicity) are observed with the GA progress(5). The measure of the cerebellar transverse diameter (CTD) is considered as a good parameter for predicting the GA and early detecting intrauterine growth restriction (IUGR)(6–8). However, the measurement of the volume of the cerebellum seems to be the most objective method for detecting cerebellar hypoplasia. The cerebellum is a small, characteristically shaped organ, so the measurement of its volume by means of two-dimensional ultrasound (2DUS), multiplying the largest diameter by a constant (0.52), involves substantial errors(9). The first study determining reference intervals of the fetal cerebellar volume by means of three-dimensional ultrasound (3DUS) was published early in the current decade. In this study performed with the Taiwanese population, utilizing the multiplanar method for volumetric calculation, it was observed that the cerebellar volume is of significance for detection of hypoplasia and genetic syndromes(10). In the recent years, a new technique for volumetric calculation with 3DUS has been utilized: the Virtual Organ Computer-Aided AnaLysis (VOCAL™), a software designed as a 3D-mode function of the SonoView Pro™ application (Medison Co., Ltd.; Seoul, Korea). An experimental in vitro study has demonstrated that this technique is more accurate than the multiplanar technique for volumetric calculation of irregularly-shaped objects(11), with recent in vivo evidence of reproducibility(12). Recently, our group performed a longitudinal study of fetal cerebellar volume between 20 and 32 weeks, utilizing the VOCAL™ method, and evidencing that the equation for determining the fetal cerebellum volume by means of the 3D ultrasound method described by Chang et al.(10) presents a lower accuracy in the Brazilian population, possibly because of remarkable ethnic differences between the studies´ populations(13). In the last two years, a new technology has been implemented into the ultrasound system Accuvix XQ (Medison Co., Ltd.; Seoul, Korea); the so called Three-dimensional eXtended Imaging (3D XI™), including the following image processing applications: Multi-Slice View (MSV), Volume CT View (VCTV) and Oblique View (OBV). The MSV allows simultaneous display of multiple sequential parallel planes with a more precise volumetric assessment, the VCTV allows multiple examinations on multiple regions of interest, while the OBV mode allows examination of a non-standard straight or curved plane in a region of interest. There is only one study in the literature evaluating the applicability of this new technology in the evaluation of malformations of the fetal central nervous system(14). The present updating paper is aimed at describing the application of the VOCAL™ and 3D XI™ methods in the evaluation of the fetal cerebellum and their potential advantages, besides describing the newest developments in this field.
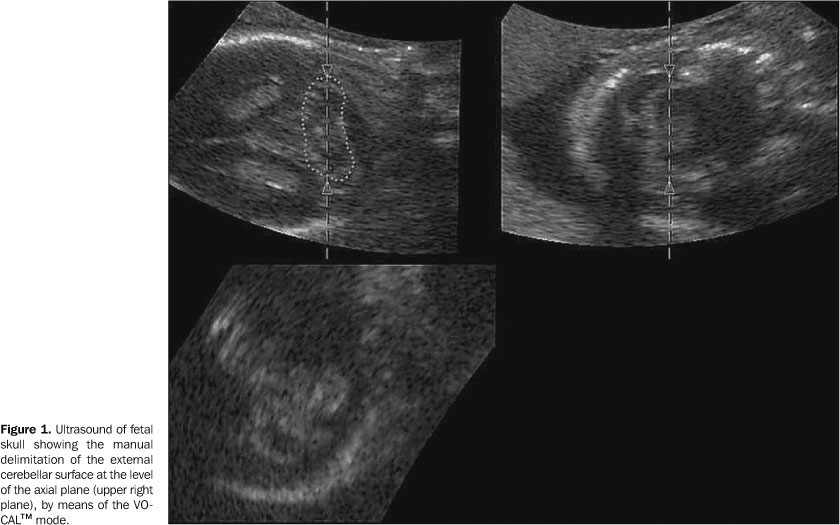
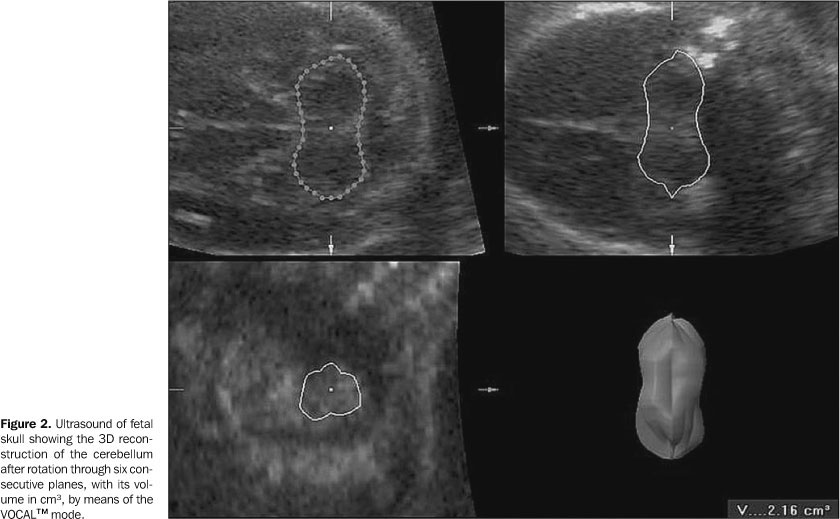
VOCAL™ METHOD The VOCAL™ mode is a software for volumetric calculation available in some ultrasound devices. This method allows a rotational movement of the structure to be analyzed around its axis, with consecutive planes being gradually displayed on the monitor screen. Image calibrators define the structure poles and the manual method or the sphere mode is utilized for delimiting external surfaces. The rotational movement can be performed at six-degree, nine-degree, 15-degree, or 30-degree intervals; that is to say at six-degree intervals, 30 consecutive planes will be delimited, and rotational movements at 30º intervals will define six consecutive planes. An area for each of these planes is calculated by the device, and, at the end of the rotational process, the volume is automatically calculated by the software, and a reconstructed 3D image of the structure is generated. As regards the literature, only the study developed by our group is found evaluating the cerebellar volume by means of the VOCAL™ method. It is a longitudinal prospective study including 52 normal pregnant women at a gestational age between 20 and 32 weeks. Fetal cerebellar volumes were obtained through 139 measurements, and an equation was defined by means of polinomial regression for predicting the cerebellar volume in relation to the gestational age. Applying the same equation for predicting the fetal cerebellum volume described for the Taiwanese population10), we have found a lower accuracy in the Brazilian population, possibly because of remarkable ethnic differences between both populations(13). Demonstration of the VOCAL™ method in the volumetric evaluation of the fetal cerebellum The cerebellum volume measurement is performed during a period of fetal rest, with a convex volumetric probe (C3-7ED) coupled with a SA-8000Live equipment (Medison Co., Ltd.; Seoul, Korea), with automatic sweeping. The sweeping is performed in real time to obtain the standard plane for measuring the TCD, as described by Goldstein et al.(3), i.e., a cutting plane parallel to the lateral ventricles taking the thalamus, the cavum septi pellucidi and the third ventricle as a reference. Posteriorly, a 3D sweeping is performed at a regular velocity (60° angle, automatically, in four seconds), obtaining the multiplanar and surface reconstruction modes. In the multiplanar mode, the sonographic image is presented into three different orthogonal planes: longitudinal plane (on the upper left corner of the screen), a transverse plane (on the upper right corner of the screen), and a frontal plane (or coronal – on the lower left corner of the screen). Whenever possible, a posterior (occipital) view is tried in order to minimize the occurrence of posterior shadowing from the temporal bones. After that, the VOCAL key is selected, with a 30º rotation angle, and the structure poles are defined with the aid of a measurements calibrator. The manual mode for the organ outlining is selected, allowing the definition of an area (Figure 1). The structure is rotated around its axial axis through six consecutive planes, and, at the end of the rotational process, the software automatically provides a 3D volumetric image of the organ with its volume in cm³ (Figure 2).
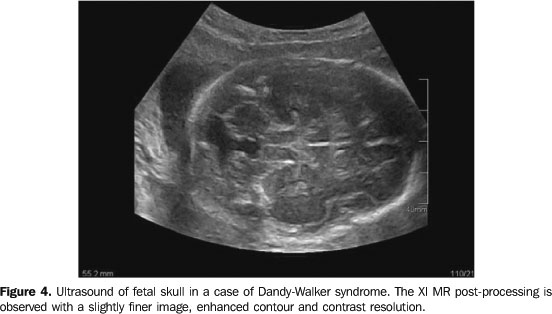
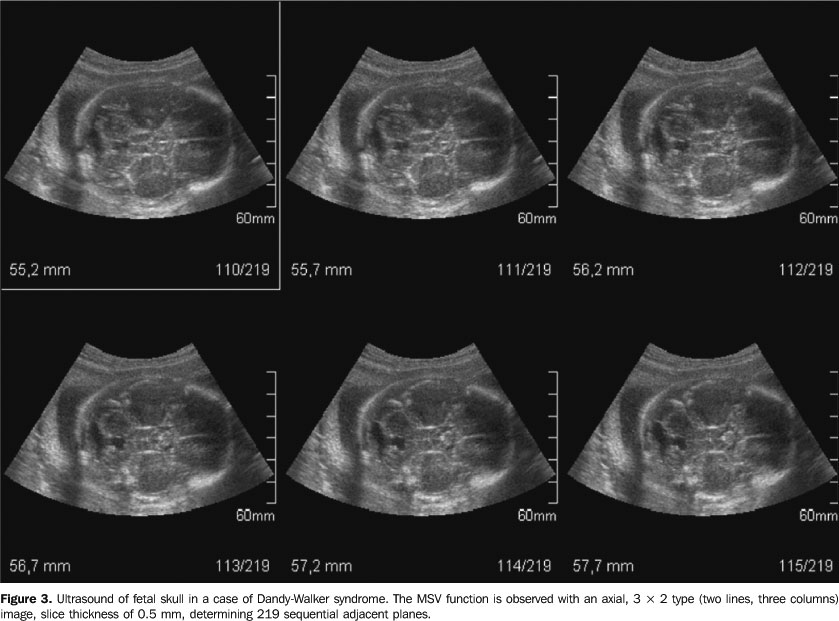
3D XI™ METHOD The 3D XI™ is a software package developed for the Accuvix XQ ultrasound system, and also is available as an optional item for the Sonoace 8000Live and 9900 systems. This package includes three applications: MSV, VCTV and OBV. The MSV application also includes an image post-processing system named Dynamic MR (XI MR), allowing a slightly finer image, with enhanced contour and increased contrast resolution. Demonstration of the 3D XI method in the evaluation of the fetal cerebellum The volumetric acquisition is performed with a convex volumetric probe (C3-7ED) or an endocavitary probe (EC4-9ES). Initially, a real time scan is performed in order to define the region of interest (ROI). Then, a 3D sweeping is performed, at a 40º–60º angle, with a slow or regular scan speed. Then, the 3D XI key is selected. The MSV mode allows multiplanar, sequential slicing, the slice thickness being defined by the operator. Figure 3 demonstrates a case of cerebellar vermis agenesis (Dandy-Walker syndrome), presenting an axial, 3 x 2 type (two lines, three columns) image (A), slice thickness of 0.5 mm, determining 219 sequential adjacent planes. The MSV allows the accurate determination of the plane showing the beginning of the end of the agenesis, and as a result defining the malformation extent. Figure 4 demonstrates the same case of cerebellar vermis agenesis utilizing the image post-processing system named Dynamic MR (XI MR); fine and sharper contours of the fetal CNS structures are observed, making the cerebellar vermis agenesis more evident.
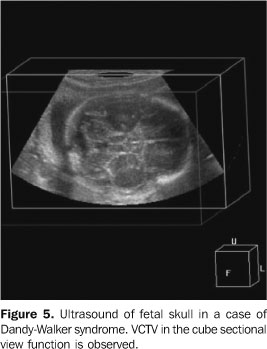
The VCTV technology with cross view (intersection between two perpendicular planes) and cube sectional view functions enables multiple examinations on multiple regions of interest. The image can be moved along the six corners of this cube (up, down, ahead, back, right and left); and also can be rotated on axes x, y and z. Figure 5 demonstrates the same case described in Figure 4, utilizing the cube sectional view function.
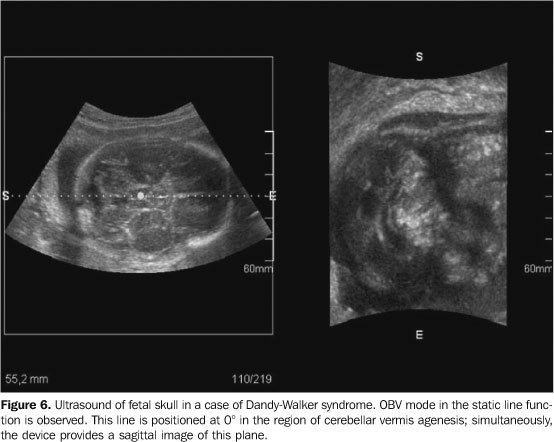
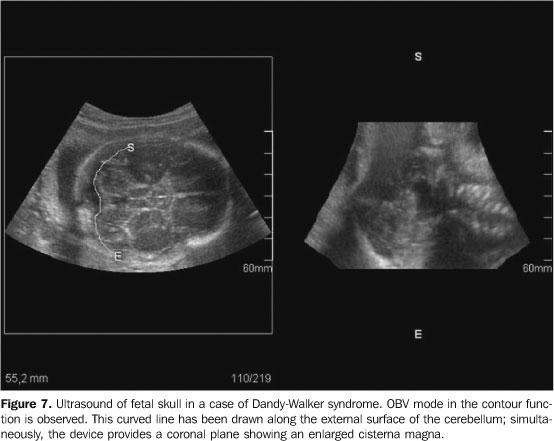
The OBV mode allows examination of a non-standard straight or curved plane in a region of interest by means of three parameters: static line, dynamic line and contour. When the static line is selected, the device automatically presents a perpendicular and central line, the ROI, and this line can be manually rotated up to 360°, generating multiple planes. Through the dynamic line, the operator selects the site on the ROI for defining the plane of interest, and, in the same way of the static line, the dynamic line also can be rotated up to 360º. On its turn, the contour function allows the obtention of structural planes with irregular contours. Figure 6 demonstrates the OBV in the static line function in a case of cerebellar vermis agenesis. This line is positioned at 0° in the region of the vermis agenesis (ROI); simultaneously, the device provides a sagittal image of this plane Figure 7 demonstrates the OBV in the contour function, with delimitation of a curved line at the level of the hemispheres and cerebellar vermis; simultaneously, the device display a plane resulting from this contour.
CONCLUSIONS The 3D US shows to be a promising method to evaluate the fetal central nervous system, especially the fetal cerebellum. The VOCAL™ method allows an accurate estimate of the cerebellar volume, an extremely significant factor in the diagnosis of growth disorders and congenital anomalies. The 3D XI™ method with the MSV mode allows the accurate determination of the plane showing the agenesis as well as its extent. The Dynamic MR allows a more clear and detailed analysis of the area of agenesis, while OBV allows examination of any nonstandard straight or oblique plane in a region of interest.
REFERENCES 1. Junqueira LCU, Zago D. Fundamentos de embriologia humana. 2ª ed. Rio de Janeiro, RJ: Guanabara Koogan, 1977;177–198. [ ] 2. Machado A. Neuroanatomia funcional. 2ª ed. Rio de Janeiro, RJ: Atheneu, 1993;49–53. [ ] 3. Goldstein I, Reece EA, Pilu G, Bovicelli L, Hobbins JC. Cerebellar measurements with ultrasonography in the evaluation of fetal growth and development. Am J Obstet Gynecol 1987;156: 1065–1069. [ ] 4. Babcook CJ, Chong BW, Salamat MS, Ellis WG, Goldstein RB. Sonographic anatomy of the developing cerebellum: normal embryology can resemble pathology. AJR Am J Roentgenol 1996; 166:427–433. [ ] 5. Hashimoto K, Shimizu T, Shimoya K, Kanzaki T, Clapp JF, Murata Y. Fetal cerebellum: US appearance with advancing gestational age. Radiology 2001;221:70–74. [ ] 6. Reece EA, Goldstein I, Pilu G, Hobbins JC. Fetal cerebellar growth unaffected by intrauterine growth retardation: a new parameter for prenatal diagnosis. Am J Obstet Gynecol 1987;157:632–638. [ ] 7. Lee W, Barton S, Comstock CH, Bajorek S, Batton D, Kirk JS. Transverse cerebellar diameter: a useful predictor of gestational age for fetuses with asymmetric growth retardation. Am J Obstet Gynecol 1991;165(4 Pt 1):1044–1050. [ ] 8. Vinkesteijn ASM, Mulder PGH, Wladimiroff JW. Fetal transverse cerebellar diameter measurements in normal and reduced fetal growth. Ultrasound Obstet Gynecol 2000;15:47–51. [ ] 9. Chang CH, Chang FM, Yu CH, Ko HC, Chen HY. Three-dimensional ultrasound in the assessment of fetal cerebellar transverse and antero-posterior diameters. Ultrasound Med Biol 2000;26:175–182. [ ] 10. Chang CH, Chang FM, Yu CH, Ko HC, Chen HY. Assessment of fetal cerebellar volume using three-dimensional ultrasound. Ultrasound Med Biol 2000;26:981–988. [ ] 11. Raine-Fenning NJ, Clewes JS, Kendall NR, Bunkheila AK, Campbell BK, Johnson IR. The interobserver reliability and validity of volume calculation from three-dimensional ultrasound datasets in the in vitro setting. Ultrasound Obstet Gynecol 2003;21:283–291. [ ] 12. Ruano R, Martinovic J, Dommergues M, Aubry MC, Dumez Y, Benachi A. Accuracy of fetal lung volume assessed by three-dimensional sonography. Ultrasound Obstet Gynecol 2005;26: 725–730. [ ] 13. Araujo Júnior E, Guimarães Filho HA, Pires CR, Nardozza LM, Moron AF, Mattar R. Validation of fetal cerebellar volume by three-dimensional ultrasonography in Brazilian population. Arch Gynecol Obstet 2007;275:5–11. [ ] 14. Kalache KD, Eder K, Esser T, et al. Three-dimensional ultrasonographic reslicing of the fetal brain to assist prenatal diagnosis of central nervous system anomalies. J Ultrasound Med 2006;25: 509–514. [ ]
Received April 11, 2005.
* Study developed in the Unit of 3D Ultrasonography of Obstetrics Department at Universidade Federal de São Paulo (Unifesp-EPM), São Paulo, SP, Brazil. |
|

{kind=link}
{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554