Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 3 - May / June of 2007
Vol. 40 nº 3 - May / June of 2007
|
ORIGINAL ARTICLE
|
|
Effects of radiotherapy on bone tissues |
|
|
Autho(rs): Samantha Seara Da Cunha, Viviane Almeida Sarmento, Luciana Maria Pedreira Ramalho, André Carlos de Freitas, Darcy de Almeida, Maria Eulina Tavares, Jaílton Caetano Souza, Elaine Bauer Veeck, Nilza Pereira da Costa |
|
|
Keywords: Radiotherapy, Ionizing radiation, Bone tissue |
|
|
Abstract:
INTRODUCTION According to data from The World Health Organization (WHO)(1), more than 11 million people are diagnosed with cancer each year, with estimated 16 million new cases per year as from 2020. Besides, cancer annually causes seven million deaths, that is to say, 12.5% of deaths in the world. Amongst therapeutic modalities, radiotherapy represents a well established method for treatment of head and neck cancer. Approximately 50% of patients with cancer are submitted to radiotherapy at some phase of their treatment, either isolatedly or in association with other forms of oncologic therapy(2). Although being frequently observed in the treatment of malignant tumors, the use of high radiation doses may generate undesirable side effects, since ionizing radiation cannot differentiate tumor cells from healthy cells(3,4). Consequently, the destruction of healthy tissues is a factor limiting the comprehensive utilization of radiation therapy. As with other tissues, bones also are affected by the radiation effects, resulting in a significant change of the bone regeneration capacity when it is injured(4,5). One of these alterations would be a disorder in the balance between the osteoblastic and osteoclastic activities, leading to a bone destructive process. Also, a decrease in the number of osteocytes and osteoblasts may be observed following the tissue irradiation. Significant post-radiation alterations of the bone matrix develop slowly, the initial changes being a result from an injury to the bone remodeling system, i.e., osteoblasts, osteocytes and osteoclasts. Osteoblasts tend to be more sensitive than osteoclasts, therefore an increase in the cellular lysis may occur(6). As a result, the process of bone matrix formation stops, hindering the mineralization process, which may lead to a spontaneous bone fractures and osteoradionecrosis(7–9). Endothelial cells also are heavily affected, and the vascular fibrosis results in a decrease in the vascularization, affecting the bone and medullary cells vitality, so the area remains susceptible to infection and necrosis, even after a small trauma(5,9). For this reason, dental extractions are contraindicated during an one-year period following radiotherapy(10). The severity of the tissue lesion will depend on the total radiotherapy dose, the effective biological dose, the size of the radiation field, the number of radiotherapy sessions and the interval between them, the dose fractioning, and the surgical and/or traumatic aggression to the irradiated tissue. Severe cases of tissue destruction usually are associated with doses > 7,000 cGy, although 6,000 cGy may result in mandible osteoradionecrosis(11,12). The present study was aimed at evaluating the radiotherapy effects on bone tissues, and the accuracy of the measurement of gray levels on radiographic images as a predictor of histological alterations of bone tissues in animal models.
MATERIALS AND METHODS The present study utilized four male, adult, clinically healthy rats Rattus norvegicus albinus, Rodentia, Mammalia, of the lineage Wistar, weighing about 210–260 g. These animals were kept in individual cages measuring 20 cm × 30 cm × 13 cm, at 22°C room temperature, luminosity (12-hour day/12-hour night cycle), 50% relative humidity, and received commercial rodents diet (Nuvilab® CR 1) and water ad libitum. All of the animals were submitted to general anesthesia by intraperitoneally injected sodic thiopental in the dosage 0.2 ml/100 g. Then the rats underwent trichotomy on their back legs coxofemoral region, and were immobilized during the irradiation procedure by means of an especially developed acrylic device based on an experiment performed by Machado(13). The animals were submitted to a single session of ionizing radiation from a cobalt-60 source, with a total of 3,000 cGy delivered to a 2 cm × 2 cm area of their right legs, utilizing only one irradiation field from the top to the bottom. The rest of the animal body was protected by lead blocks inserted into the radiotherapy device. The animals were sacrificed six weeks after radiotherapy, and both irradiated and non-irradiated legs were dissected. The animals' legs were placed with their ventral surfaces directly onto an imaging plate for cephalometric radiography of a DenOptix® (300 dpi, pixel de 85 µm) digital radiographic system. A five-step aluminium wedge with 1 mm increment was added to the apparatus. The radiographic device (Timex® – 70 kV e 7 mA) was set for 0.06 s exposure time, 1.20 cm focal distance and perpendicular beam. After the radiographic exposure, the plate was read by the DenOptix® system, allowing the generation of the corresponding digital images which were exported and stored as bitmap files. These files are opened in the Photoshop® application for brightness correction with basis on the penetrometer and saved again. After that, the images were opened with the Image Tool® software, and a polygon was traced on the irradiated region of each rat. The mean gray level was measured by the "histogram" tool. So the mean gray levels measured for each specimen were compared (Student-t test). Then the specimens were longitudinally incised to expose the whole femur whose thickness was measured with a digital Starrett 727 series pachymeter and a Zeiss® magnifying glass. The femurs were sent for histological processing and hematoxylin-eosin and picrosirius red staining. The following parameters were analyzed on the histological slides: presence of collagen fibers, level of periosteal osteoblastic activity, degree of bone reabsorption near the medulla, and amount of adipous tissue. The latest three items were evaluated as for their intensity degree as follows: mild intensity, grade 1; moderate intensity, grade 2; severe intensity, grade 3. These results were evaluated by means of the non-parametric chi-square test (error probability, 5%). Additionally, a counting of the number of osteocytes and Haversian canal was performed in 10 fields. Such results were analyzed by means of the non-parametric Kruskal-Wallis test (error probability, 5%).
RESULTS After the femurs thickness measurement, a lower thickness was observed on the irradiated legs (4.20 mm × 2.84 mm) as compared with the non-irradiated legs (4.67 mm × 3.11 mm). This value was statistically significant (p < 0.05). Regarding the digital radiographic analysis, it was possible to observe that, in the irradiated legs, the bone tissue amount was smaller (mean gray levels, 118) as compared with the nonirradiated legs (mean gray level, 123.5), but this difference was not statistically significant (p > 0.05) (Figure 1).
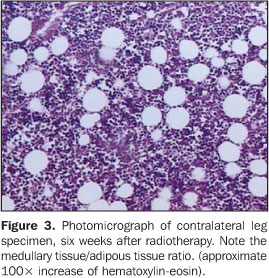
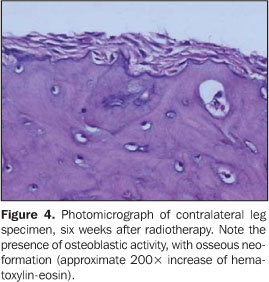
Histologically, the irradiated legs presented a high amount of adipous tissue and, consequently, a decrease in the amount of medullary tissue (Figure 2). A low index of osteoblastic activity has occurred, this activity being formed by periosteal osteoblasts. Also, areas of moderate bone reabsorption were observed. This osteoclastic activity was characterized by the presence of lacunae of cortical bone reabsorption near the medullary portion. Collagen fibers were found in 50% of specimens. A counting demonstrated a marked scarcity of osteocytes. The same has occurred with the Haversian canals. Also on the contralateral, non-irradiated legs, a low number of osteocytes were found, but the difference between the irradiated and non-irradiated legs (p > 0.05) was not statistically significant. The same has occurred with the counting of Haversian canals (p > 0.05). However, as regards the adipous/medullary tissues ratio, a mild presence of fat cells, and a moderate presence of medullary tissue were observed (Figure 3). This ratio was statistically significant as compared with the irradiated legs (p < 0.05). As regards the osteoblastic activity, the non-irradiated leg presented moderate to intense activity (Figure 4), and this difference was statistically significant (p < 0.05). The presence of collagen fibers has not been observed, but this difference has not been statistically significant as compared with the irradiated leg (p > 0.05). Mild to moderate bone reabsorption has been observed, although with no statistically significant difference (p > 0.05).
DISCUSSION The animal model chosen for the present study was the rat, since it is the most utilized for evaluating secondary effects of radiotherapy in studies developed by several authors(4,9,14,15). Because of difficulties inherent to animal model studies, the rats were exposed to a single radiation dose enough to cause trabecular changes; besides, this single dose was based on protocols reported by previous studies(4,9,14–16), ranging between 25 Gy and 35 Gy. The cobalt-60 apparatus was chosen because of its higher accessibility and for knowingly causing more adverse effects than other radiation sources(17). Based on the results of digital radiographic evaluation, it is possible to infer that the method has presented a good sensitivity because, even in the absence of a statistically significant mean gray level between irradiated and contralateral legs, these results are similar to those of the histological analysis where significant differences also have not been found among some structures evaluated. The sensitivity of the evaluation of gray levels on digital radiographic images of bone tissues has already been analyzed both in other in vivo studies(18) and animal model studies(19). The literature has demonstrated that osseous alterations observed on irradiated bone are visible and are directly related to cellular scarcity in the bone structure(15). However, this assertion has been just partially evidenced with the present study, since although the irradiated bone has presented less cellularized, it cannot be affirmed that this has occurred as a result of radiotherapy, since the contralateral leg has not demonstrated statistically significant difference as regards the number of osteocytes. The same has occurred with regard to the number of Haversian canals. On the irradiated leg, a little number of Haversian canals was observed, but this number was not statistically significant in comparison with the contralateral leg. Studies developed by Morales et al.(20) have found a decreased local vascularization after exposure of rabbits mandibles to ionizing radiation. However, the animals mandibles utilized by these researchers as a comparison media, had not been submitted to any type of radiotherapy, as a comparison media. Besides these effects, a low osteoblastic activity could be observed in the irradiated leg. These findings are similar in studies developed by Matsumura et al.(21), Dare et al.(22) and Dudziak et al.(23), who have found a decrease in osteoblastic proliferation, leading to the idea that ionizing radiation implies the terminal differentiation between precursor bone cells and osteoblasts. The same fact has not occurred in the non-irradiated leg. The collagen production, however, was not affected, being observed in 50% of the irradiated legs although this finding has not been statistically significant as compared with the contralateral leg which has not presented collagen. Zones of bone reabsorption were visible, although not with the expected intensity. Once more, there was no significant difference between irradiated and non-irradiated legs. These findings go against those of Kiyohara et al.(4), who have found bone reabsorption in irradiated legs as from the fourth week after radiotherapy, with thinning of bone trabeculae. However, the bone thickness observed in the irradiated leg was statistically smaller than in the non-irradiated leg, contradicting the histological findings. This suggests that, in some moment, a possible bone reabsorption process has occurred. Also, an expressive increase in fat tissue was found, with the consequent reduction of bone marrow tissue. This fact had already been previously documented(4,15).
CONCLUSION It may be concluded that radiotherapy in the dose utilized in the present study, has determined a decrease in the bone remodeling activity in the majority of specimens evaluated, which could be radiographically detected by measuring the gray levels of the bone tissue on digital radiographic images.
Acknowledgment We thank to the Hospital Santa Izabel, for lending the hospital premises and for the devices operation.
REFERENCES 1. World Health Organization. Cancer home. Acessado em: 5/7/2005. Disponível em: http://www. who.int/cancer/en/ [ ] 2. Hyderley LJ, Maddock PG. Noções gerais da radioterapia. In: Manual de enfermagem oncológica. São Paulo: Fundação Oncocentro de São Paulo, 1996;91–97. [ ] 3. Calhoun KH, Shapiro RD, Stiernberg CM, Calhoun JH, Mader JT. Osteomyelitis of the mandible. Arch Otolaryngol Head Neck Surg 1988; 114:1157–1162. [ ] 4. Kiyohara S, Sakurai T, Kashima I. Early detection of radiation-induced structural changes in rat trabecular bone. Dentomaxillofac Radiol 2003;32: 30–38. [ ] 5. Bras J, De Jonge HK, van Merkesteyn JP. Osteoradionecrosis of the mandible: pathogenesis. Am J Otolaryngol 1990;11:244–250. [ ] 6. Vissink A, Jansma J, Spijkervet FKL, Burlage FR, Coppes RP. Oral sequelae of head and neck radiotherapy. Crit Rev Oral Biol Med 2003;14:199–212. [ ] 7. Aitasalo K. Bone tissue response to irradiation and treatment model of mandibular irradiation injury. An experimental and clinical study. Acta Otolaryngol Suppl 1986;428:1–54. [ ] 8. Mitchell MJ, Logan PM. Radiation-induced changes in bone. RadioGraphics 1998;18:1125–1136. [ ] 9. Würzler KK, DeWeese TL, Sebald W, Reddi AH. Radiation-induced impairment of bone healing can be overcome by recombinant human bone morphogenetic protein-2. J Craniofac Surg 1998; 9:131–137. [ ] 10. Németh Z, Somogyi A, Takácsi-Nagy Z, Barabás J, Németh G, Szabó G. Possibilities of preventing osteoradionecrosis during complex therapy of tumors of the oral cavity. Pathol Oncol Res 2000; 6:53–58. [ ] 11. Carlson ER, Zak MJ. Osteoradionecrosis and hyperbaric oxygen. Proceedings of the First International Congress on Maxillofacial Prosthetics 1996;184–191. [ ] 12. Jereczek-Fossa BA, Orecchia R. Radiotherapy-induced mandibular bone complications. Cancer Treat Rev 2002;28:65–74. [ ] 13. Machado RCL. Avaliação do efeito protetor da glutamina na resposta inflamatória do intestino delgado à radioterapia abdominal: estudo experimental em ratos. (Dissertação de Mestrado em Farmácia). Salvador, BA: Universidade Federal da Bahia, 2002. [ ] 14. Arnold M, Stas P, Kummermehr J, Schultz-Hector S, Trott KR. Radiation-induced impairment of bone healing in the rat femur: effects of radiation dose, sequence and interval between surgery and irradiation. Radiother Oncol 1998;48:259–265. [ ] 15. Maeda M, Bryant MH, Yamagata M, Li G, Earle JD, Chao EY. Effects of irradiation on cortical bone and their time-related changes. A biomechanical and histomorphological study. J Bone Joint Surg Am 1988;70:392–399. [ ] 16. Jacobsson M, Jonsson A, Albrektsson T, Turesson I. Dose-response for bone regeneration after single doses of 60Co irradiation. Int J Radiat Oncol Biol Phys 1985;11:1963–1969. [ ] 17. Pachigolla R, Pou A, Quinn F. The principles of radiation oncology. Grand Rounds Presentation, UTMB, Dept. of Otolaryngology, 2000. Acessado em: 10/11/2005. Disponível em: http://www. utmb.edu/otoref/Grnds/Radiation-Oncology-200001/Radiation-Oncology-200001.htm [ ] 18. Sarmento VA, Rubira IRF. Mensuração da densidade óptica apical – uma proposta para diagnóstico diferencial em endodontia. J Bras Odontol Clín, Curitiba 1998;12:65–68. [ ] 19. Sarmento VA, Pretto SM. Diagnóstico radiográfico de alterações periapicais de origem endodôntica através da determinação do nível de cinza em imagens digitais – estudo experimental em ratos. Rev Pós-Grad Fac Odontol Univ São Paulo 2003; 10:333–345. [ ] 20. Morales MJ, Marx RE, Gottlieb CF. Effects of pre- and postoperative irradiation on the healing of bone grafts in the rabbit. J Oral Maxillofac Surg 1987;45:34–41. [ ] 21. Matsumura S, Jikko A, Hiranuma H, Deguchi A, Fuchihata H. Effect of x-ray irradiation on proliferation and differentiation of osteoblast. Calcif Tissue Int 1996;59:307–308. [ ] 22. Dare A, Hachisu R, Yamaguchi A, Yokose S, Yoshiki S, Okano T. Effects of ionizing radiation on proliferation and differentiation of osteoblast-like cells. J Dent Res 1997;76:658–664. [ ] 23. Dudziak ME, Saadeh PB, Mehrara BJ, et al. The effects of ionizing radiation on osteoblast-like cells in vitro. Plast Reconstr Surg 2000;106: 1049–1061. [ ]
Received July 13, 2006.
* Study developed at Universidade Federal da Bahia (UFBA), Hospital Santa Izabel (HSI) and União Metropolitana de Educação e Cultura (Unime), Salvador, BA, and at Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554