Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 2 - Mar. / Apr. of 2007
Vol. 40 nº 2 - Mar. / Apr. of 2007
|
REVIEW ARTICLE
|
|
Relevant radiological findings for the diagnosis of necrotizing enterocolitis and its complications |
|
|
Autho(rs): Beatriz Regina Alvares, Daniel Lahan Martins, Renato Lopes Roma, Inês Minniti Rodrigues Pereira |
|
|
Keywords: Necrotizing enterocolitis, Newborn, Radiological diagnosis |
|
|
Abstract: IPhDs, Professors for Department of Radiology of Faculdade de Ciências Médicas da Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil
INTRODUCTION Necrotizing enterocolitis (NEC)represents a condition whose etiology still remains unclear,predominantly affecting neonates (NN) weighing less than 1,500 g,and is one of the most frequent and severe gastrointestinalemergencies occurring in the neonatalperiod(1–3). Most frequently accepted etiologicalfactors for explaining this condition are intestinal ischemia,resulting in alterations of the intestinal mucosa, excessivebacterial growth with formation of gas in the intestinal wall andpersistent intestinal irritation because of oral feeding. Themost suggestive clinical findings of this disease are abdominaldistension, food or bilious emesis and presence of blood instools(2,3). The abdominal plain x-ray is a routineprocedure in NN with NEC, since it plays an essential role in thediagnosis, follow-up and detection of complications indicatingthe need for surgery. During the treatment, NN should undergoserial plain x-rays every hour to allow the early diagnosis ofcomplications(4,5).
RADIOLOGICAL ALTERATIONS 1 – Generalized intestinaldistension The earliest radiological alteration in NEC is a diffused and persistent intestinal gas distension(5). Radiologically, an intestinal loop may be considered as dilated when its measure surpasses the width of the first lumbar vertebral body(6,7). This may be a non-specific radiological finding in NN with other abnormalities, especially those under continuous ventilation by positive pressure(8). Nevertheless, the suspect of NEC should be always be raised in radiological of NN presenting with persistent, generalized intestinal distension and characteristic clinical picture(2,6) (Figure 1).
2 – Localized distension of anintestinal loop Localized distension o an intestinal loop presenting a tubular configuration and thickened walls was initially described as a radiological sign of imminent perforation. Currently, this radiological sign has not been considered as an imminent risk of perforation anymore, although it is useful to raise the suspicion of NEC at its early phase, since this may mean loop distress(9,10) (Figure 2).
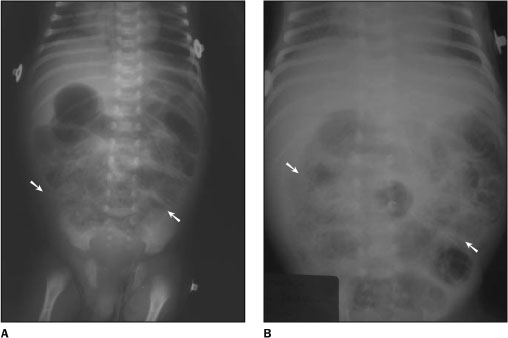
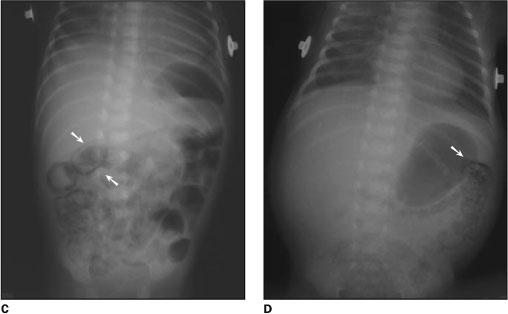
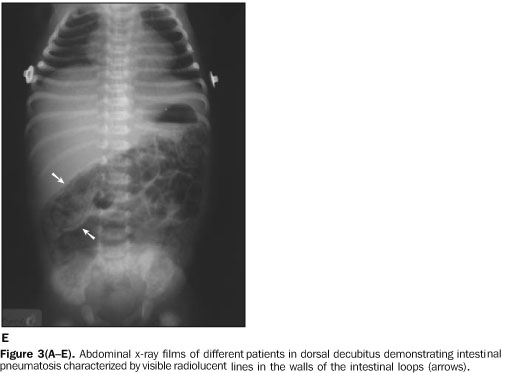
3 – Intestinalpneumatosis Pneumatosis means presence of gas in theintestinal wall, representing a complication from necrotizingenterocolitis. Although there is also a destruction of theintestinal mucosa, the presence of intramural gas is consideredas a consequence of an excessive bacterial increase with gaspassage from the intestinal lumen into the loop wall. The gas maybe in the stomach and intestine walls, but predominates in thelarge intestine wall(11). Intestinal pneumatosis represents the most pathognomonic radiological finding of NEC, presenting as visible radiolucent, linear, curved-linear or bullous images on the intestinal loop wall. In some circumstances, the radiological appearance resembles the intestinal fecal contents, and the diagnosis is made by means of serial x-rays demonstrating the permanence of intramural gas, contrarily to the feces with present motility(2,11–13) (Figure 3A–E).
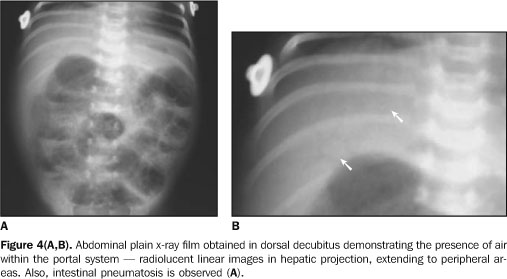
4 – Air within the portal system The intestinal pneumatosis may extend into the venous portal system, and is visible on abdominal plain x-ray films as radiolucent, linear images in hepatic projection, and extending to peripheral areas(6, 11,14,15) (Figures 4A and 4B). This type of distribution allows the differential diagnosis with air in the biliary tract, with a radiological aspect similar to that of air within the portal system, but with a more central hepatic localization(6).
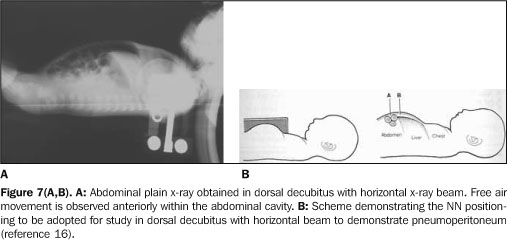
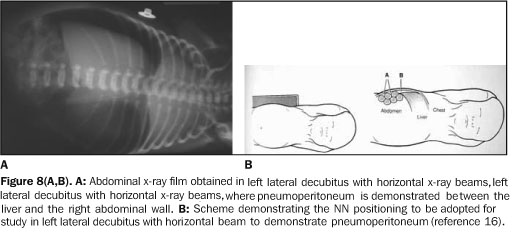
5 – Pneumoperitoneum The term pneumoperitoneum refers to thepresence of free air within the peritoneal cavity caused by aperforated hollow, and is a complication from necrotizingenterocolitis(1,2,6,11). The radiological signscan be seen on abdominal plain x-rays performed in dorsaldecubitus, with vertical and horizontal x-ray beams, orthostaticposition and left lateral decubitus with horizontalbeams(11,16). On x-ray films obtained in dorsal decubitus with vertical x-ray beams a darkened abdominal cavity is observed, and the intestinal wall is visualized because of the presence of air both inside and outside the loop (Figure 5). On this view, a falciform ligament may appear, the association of these images being described as "football sign" for resembling the shape of the ball used in the American football(11). On x-ray films obtained with the patients in orthostatic position (Figure 6), dorsal decubitus (Figures 7A and 7B) and left lateral decubitus with horizontal x-ray beam (Figures 8A and 8B), the free air movement is observed within the abdominal cavity, under the diaphragmatic cupula, anteriorly, or between the liver and the right abdominal wall.
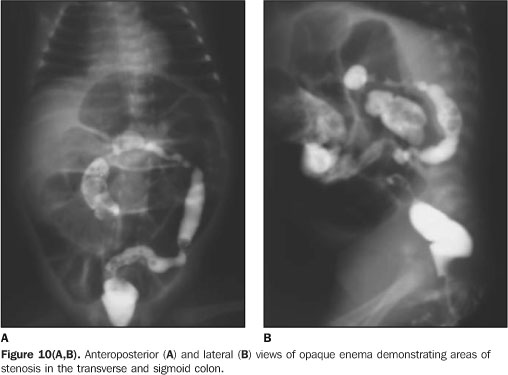
6 – Late complications Areas of stenosis of the large intestine represent a late complication from necrotizing enterocolitis, manifesting clinically through obstruction. On plain abdominal x-ray films, a significant intestinal distension is observed with absence of air in the rectum(17,18). The diagnosis is confirmed by opaque enema demonstrating areas of stenosis in the large intestine. In the presence of risk of intestinal rupture, this examination should be performed with diluted iodinated contrast agent(18,19) (Figures 9, 10A and 10B).
CONCLUSION The radiological diagnosis of NECaccomplished in all phases contributes for an immediatetherapeutical management, reducing the rate of complications andimproving the patients' survival.
REFERENCES 1. Kosloske AM, Musemeche A. Necrotizing enterocolitis of the neonate. Clin Perinatol 1989;16:97–111. [ ] 2. Buonomo C. The radiology of necrotizing enterocolitis. Radiol Clin North Am 1999;37:1187–1198. [ ] 3. Ostlie DJ, Spilde TL, St Peter SD, et al. Necrotizing enterocolitis in full-term infants. J Pediatr Surg 2003;38:1039–1042. [ ] 4. Kanto Jr WP , Hunter JE, Stoll BJ. Recognition and medical management of necrotizing enterocolitis. Clin Perinatol 1994;21:335–346. [ ] 5. Daneman A, Woodward S, da Silva M. The radiology of neonatal necrotizing enterocolitis (NEC). A review of 47 cases and the literature. Pediatr Radiol 1978;7:70–77. [ ] 6. Morrison SC, Jacobson JM. The radiology of necrotizing enterocolitis. Clin Perinatol 1994;21: 347–363. [ ] 7. Edwards DK. Size of gas-filled bowel loops in infants. AJR Am J Roentgenol 1980;135:331–334. [ ] 8. Jaile JC, Levin T, Wung JT, Abramson SJ, Ruzal-Shapiro C, Berdon WE. Benign gaseous distention of the bowel in premature infants treated with nasal continuous airway pressure: a study of contributing factors. AJR Am J Roentgenol 1992; 158:125–127. [ ] 9. Wexler H. The persistent loop sign in neonatal necrotizing enterocolitis: a new indication for surgical intervention? Pediatr Radiol 1978;126:201–204. [ ] 10. Leonard Jr T , Johnson JF, Pettett PG. Critical evaluation of the persistent loop sign in necrotizing enterocolitis. Radiology 1982;142:385–386. [ ] 11. Swischuk LE. Alimentary tract. In: Swischuk LE, editor. Imaging of the newborn, infant, and young child. 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2004;341–589. [ ] 12. Heng Y, Schuffler MD, Haggitt RC, Rohrmann CA. Pneumatosis intestinalis: a review. Am J Gastroenterol 1995;90:1747–1758. [ ] 13. Pear BL. Pneumatosis intestinalis: a review. Radiology 1998;207:13–19. [ ] 14. Molik KA, West KW, Rescorla FJ, Scherer LR, Engum SA, Grosfeld JL. Portal venous air: the poor prognosis persists. J Pediatr Surg 2001;36: 1143–1145. [ ] 15. Briski LE, Von Berg V, Humes JJ. Necrotizing enterocolitis of the newborn. Ann Clin Lab Sci 1982;12:186–193. [ ] 16. Gyll C. The abdomen. In: Meerstadt PWD, Gyll C, editors. Manual of neonatal emergency x-ray interpretation. London: Saunders, 1994;152–237. [ ] 17. Virgee JP, Gill JG, Desa D, Somers S, Stevenson GW. Stricures and other late complications of neonatal necrotizing enterocolitis. Clin Radiol 1979;30:25–31. [ ] 18. Kao SCS, Smith WL, Franken Jr EA, Sato Y, Sullivan JH, McGee JA. Contrast enema diagnosis of necrotizing enterocolitis. Pediatr Radiol 1992;22:115–117. [ ]
Received March 29, 2005.
* Study developed in the Department of Radiology of Faculdade de Ciências Médicas da Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil. |
|






Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554