Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 41 nº 5 - Sep. / Oct. of 2008
Vol. 41 nº 5 - Sep. / Oct. of 2008
|
ORIGINAL ARTICLE
|
|
Evaluation of radiation exposure to physicians during hemodynamic interventional procedures |
|
|
Autho(rs): Leonardo Peres da Silva, Claudia Lúcia de Pinho Maurício, Lucía Viviana Canevaro, Paulo Sérgio Oliveira |
|
|
Keywords: Interventional radiology, Fluoroscopy, Hemodynamic procedures, Radiation protection, Thermoluminescent dosimetry |
|
|
Abstract:
IMaster, Medical Physicist in Radiotherapy, Substitute Professor, Department of Radiology - Faculdade de Medicina da Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
INTRODUCTION Interventional radiology involves imaging-guided percutaneous diagnostic and/or therapeutic interventions. Generally, these procedures are performed under local anesthesia and/or sedation. Fluoroscopy is utilized for localizing a lesion or site for treatment, monitoring a procedure, and documenting a therapy(1). Radiopaque substances known as contrast means are utilized for visualization of radiotransparent organs or tissues on a monitor display. These procedures are absolutely justifiable both for patients and health systems, considering that these interventions replace complex surgeries with other simpler medical procedures, reducing risks and inpatients stay in the hospital, as well as the overall cost of the procedure. However, interventional radiology is one of the specialties in medical radiology where the practitioner is exposed to the highest radiation doses(2). Occupational doses are high, and some deterministic radiation effects, such as cataract and extremities hair loss, have been already identified in interventional physicians(1,3). Such high doses result from the medical staff members, especially the interventional physician proximity with the patient and the x-ray tube. Mobile protective screens between the physician and the patient, and personal protection clothes should be utilized in order to reduce radiation exposure(4). The main personal protection clothes are the following: lead aprons, thyroid collars, leaded glasses and radiation protection gloves. It is important to note that practitioners involved in procedures performed in interventional radiology rooms are cardiologists, orthopedists, vascular surgeons, neurologists, etc., who generally have not underwent education in radiological protection. This education is becoming critical for those practitioners involved in the utilization of dedicated x-ray equipment, among other reasons, because of the progressive technological sophistication. In Brazil, the Portaria (Order) 453/98 of the Ministry of Health(5) establishes the radiological protection guidelines for medical and odontologic radiology. Such regulation defines the radiological protection requirements for licensing and control of radiology services, including those operating with fluoroscopy. These guidelines include both Comissão Nacional de Energia Nuclear (CNEN) and international baseline principles(6,7): 1. Justification for the practice and medical personal exposure to radiation; 2. Radiological protection optimization; 3. Limitation of individual occupational and public doses. The practice of interventional radiology as diagnostic and therapeutic means is absolutely justifiable; however, aspects related to the optimization of this practice still require additional studies, evaluations and implementation. The Portaria (Order) 453/98 regulates especially aspects related to the practice of conventional radiology and fails in presenting specific requirements regarding interventional radiology. Monthly individual monitoring is required in the follow-up of the working conditions of all practitioners involved in procedures of medical radiology in order to estimate the effective dose and, in some cases, the dose-equivalent in the crystalline and extremities. The "effective dose" is the amount corresponding to the estimated total risk for induction of stochastic effects resulting from radiation exposure. "Equivalent dose in an organ or tissue" corresponds to the mean absorbed dose in such an organ or tissue multiplied by a weighting factor associated with the type of radiation. For photons, this weighting factor is = 1. The mean annual effective dose received by the practitioner should not exceed 20 mSv in any consecutive five-year period, and not exceeding 50 mSv/year. The annual dose-equivalent should not exceed 500 mSv for skin and extremities, and 150 mSv for the crystalline. Effective doses > 1.5 mSv/month should be investigated. When a lead apron is utilized, the personal dosimeter should be placed over the apron, located at the most exposed region of the chest, with the measurement value being divided by a correction factor = 10 for estimating the effective dose. The measurement value should be interpreted as the dose-equivalent in unshielded regions of the body. In cases where extremities and/or eyes are subject to doses significantly higher than the reading of the personal dosimeter on the chest, additional dosimeters should be utilized. All the measurements should be performed with the "personal dose-equivalent", Hp(d), that is the operational measure of external personal monitoring, defined as the absorbed dose in a point at a depth d, measured in millimeters, of the body, in soft tissues, multiplied by the radiation quality factor that, in the case of x-rays is 1. For the chest, d = 10 is utilized; for extremities, d = 0.07 mm; and for the crystalline, d = 3 mm. Currently, interventional radiology has been widely utilized in cardiology, and is called interventional cardiology. The doses received by the practitioners involved in interventional cardiology procedures depend on different factors such as clinical and technical characteristics for each procedure, experience of the interventional cardiologist, training in radiological protection, utilization of personal protection clothes, knowledge of the correct x-ray equipment functioning and the positioning of the physician in relation to the x-ray equipment and the patient(8). In the present study, the influence of some factors on the dose received by interventional physicians during procedures of coronariography and coronary angioplasty was investigated, with the intention of contributing for the optimization of the occupational radiological protection in this activity. These two procedures were selected for being the most frequently performed in the hospital evaluated.
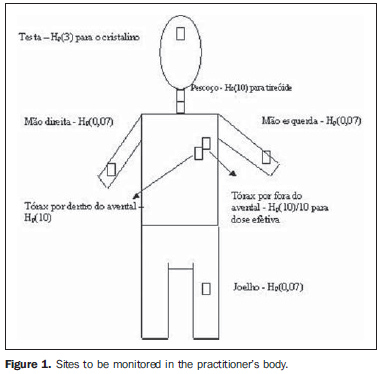
MATERIALS AND METHODS Practitioners working in three rooms of hemodynamics of a school hospital in Rio de Janeiro, RJ, Brasil, were followed-up during coronary angioplasty procedures (30) and coronariography procedures (60). Typically, a responsible physician (senior), a physician assistant (junior), a nurse and a technician remain in the room during these procedures. During angioplasty, also an anesthetist is always present. Each practitioner performs about 1,000 procedures a year. The procedures were performed with the following x-ray equipment: two 3-phase Siemens Coroskop Hip Top (Siemens AG; Munich, Germany), continuous and pulsed radiation modes with 7.5, 15 and 30 f/s, x-ray tubes with up to 150 kV, additional 0.2 mm copper filtration for fluoroscopy, x-ray image intensifier with field of 13, 17 and 23 cm2, normal and high air kerma rate respectively denominated fluoro and fluoro+; one 3-phase GE Arcomax CGR (General Electric Medical Systems; Milwaukee, USA), table Angix 80, continuous radiation mode with x-ray tube of up to 150 kV, low, normal and high air kerma rates, and image intensifier with fields of 15, 23 and 30 cm2. Thermoluminescent dosimeters (TLDs) TLD100 (LIF:Mg,Ti) (Harshaw) with chips of 3 x 3 x 0.5 mm3, supplied by Laboratório de Dosimetria Termoluminescente (LDT) (Laboratory of Thermoluminescent Dosimetry) of Instituto de Radioproteção e Dosimetria (IRD) were utilized in the present study. These dosimeters were selected particularly because of their low power dependence, linearity throughout the whole range of expected dose values, and good stability(8). The TLDs were packed in black plastic bags (for light-shielding and protection). These plastic bags were attached with surgical tape to seven sites of the body of the practitioners involved in interventional procedures: two on the chest (under and over the lead apron), two on the hands (one on the right wrist and other on the left), one on the forehead, on the left knee, and one on the neck. Figure 1 shows the seven sites evaluated.
The dosimeter placed on the chest, under the apron, estimates the dose to the organs shielded by the apron. The site on the forehead is utilized for estimating the dose to the crystalline, Hp(3), the dosimeter on the knee estimates the dose to the lower extremities, Hp(0.07), and on the hands, the dose to the upper extremities, Hp(0.07). The dosimeter of the neck estimates the dose to the thyroid, Hp(10). Measurements of doses to the thyroid (neck) were performed in practitioners with and without thyroid collar during the procedures. In cases where the practitioner utilized a thyroid collar, the TLD was placed under this accessory. The dosimeter placed over the apron on the chest estimates the dose to the unshielded regions of the body, and, by dividing its response by 10, the effective dose. The measurements were performed for each procedure and only the physician who performed the procedure was evaluated. Overall, five different physicians were evaluated in 30 angioplasty and 60 coronariography procedures. Some coronariography procedures were performed in the pulsed mode, while others were performed in the continuous fluoroscopy mode (real time imaging). In both x-ray systems, the digital mode was utilized for images acquisition (recorded image). The GE Arcomax CGR equipment was adapted to replace the cine mode with the digital mode for images acquisition. So, a comparison could be performed among the doses received by the practitioners on their hands, eyes and knees in these three modes. Brachial access (through the arm) was utilized in some of the procedures described in the present study to achieve the vein or artery for the catheter introduction, and femoral access (through the inguen) in other. A comparison was performed between the doses received by the practitioners involved in these procedures by both access pathways.
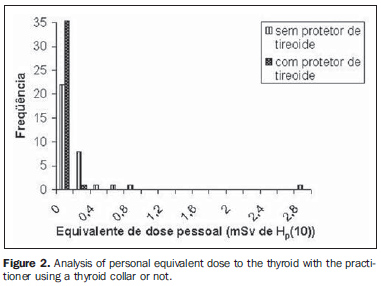
RESULTS Figure 2 presents the distribution of the values measured for Hp(10) on the neck of the practitioners with and without thyroid collar.
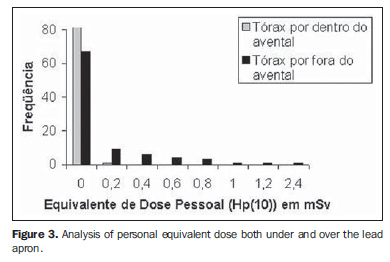
Figure 3 presents a comparison between results of measurements performed with the dosimeters under and over the lead apron.
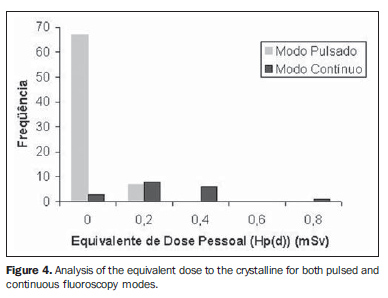
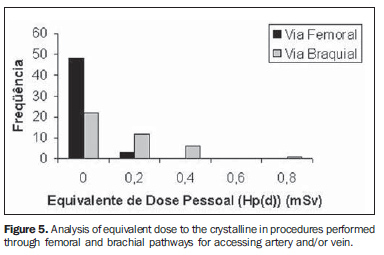
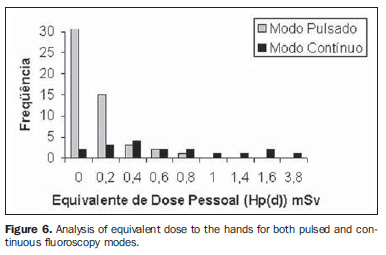
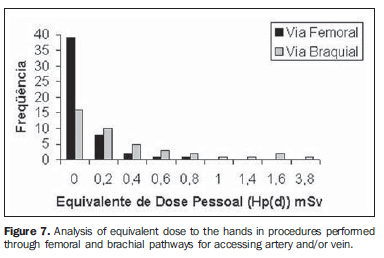
Figures 4, 5, 6 and 7 show the distribution of the values corresponding to dose-equivalent on the hands and eyes of the practitioners who performed the procedures through brachial and femoral pathways and in the pulsed and continuous fluoroscopy modes.
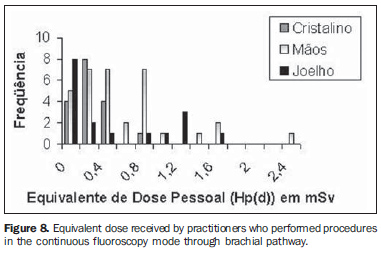
Some coronariography procedures were performed through brachial pathway and continuous mode. Figure 8 shows the dose-equivalent on the hands, crystallines and knees of the physicians Who performed the procedures combining both techniques (continuous mode + brachial access).
DISCUSSION In the physicians' thyroid monitoring, the highest dose-equivalent values were obtained in cases where the practitioner did not use the thyroid collar, clearly demonstrating the significant role played by these protectors in the reduction of the dose. The highest equivalent dose received by the practitioners who used the thyroid collar was 0.3 mSv, while without the protector this value achieved 2.9 mSv during one procedure. The reading for Hp(10) on the dosimeter under the apron represents the dose received by the practitioner on this site. This comparison is aimed at evaluating the difference between the dose over the apron multiplied by the apron attenuation factor (0.1) and the dose under the apron. The highest Hp(10) value measured over the apron was 2.4 mSv which, once divided by ten (or multiplied by 0.1), will result in a maximum value of 0.24 mSv, within the range of values measured by the dosimeter under the lead apron. The doses to the eyes, hands and knees of the practitioners who performed the procedures described in the present study presented a wide variation according to the pathway utilized for accessing the vein and/or artery catheter introduction, and the fluoroscopy mode utilized (continuous or pulsed). The practitioners involved in the procedures through brachial pathway received higher doses than those who performed the procedures through femoral pathway, as a result of the positioning of the practitioner during the procedure, considering that during the procedure through brachial pathway the physician is closer to the x-ray tube than during the procedure through femoral pathway.(9) The values for dose-equivalent evaluated on the hands, eyes and knees of practitioners who performed coronariography procedures in the continuous mode were, on average, higher than the values in the fluoroscopy pulsed mode. Dose values on Figures 4 to 8 indicate the necessity of leaded glasses for protection of the crystalline and additional personal protection on the extremities, particularly the hands, considering that they were the sites where the highest doses were found. The values for doses to the crystalline and extremities multiplied by the annual workload might exceed the annual dose threshold established for these anatomical regions and likely to induce future complications. For example, the average of doses to the crystalline under these conditions, 0.35 mSv, multiplied by a workload of 1,500 procedures/year corresponds to a dose-equivalent of 0.52 Sv, exceeding the dose standard threshold of 0.5 Sv(10) recommended to avoid formation of opacity in the crystalline lens. As far as the fact that the chest is the most exposed region of the body is concerned, the utilization of only a single dosimeter on the chest is appropriate. Considering that, during interventional cardiology procedures, other parts of the body, particularly the hands, are subject to higher radiation doses as shown on Figures 4-8, the present study recommends the utilization of additional dosimeters for these regions.
CONCLUSIONS The results of the present study clearly demonstrate the relevance of the utilization of thyroid collars, besides lead apron, by every interventional physician during all the procedures. The dose over the apron multiplied by the apron attenuation factor (0.1) is close to the dose under the apron. The doses to the hands, crystalline and knees of the practitioners who performed interventional procedures through the brachial pathway and in the fluoroscopy continuous mode were higher than the doses in procedures through the femoral pathway and in the fluoroscopy pulsed mode. The dose to these sites multiplied by the annual workload could exceed the standard threshold for these anatomical regions. In this case, the adoption of additional protective measures is required. In order to reduce the doses received by interventional physicians, it is necessary to implement mechanisms of training in radiation protection for practitioners involved in interventional cardiological procedures, additionally to the implementation of a quality control process for x-ray equipment(11). All these practitioners must be aware that, additionally to lead aprons, it is essential for them to utilize other personal protection clothes, such as thyroid collars, leaded glasses and protection gloves(4). In the market, there are special protection gloves made of other material than lead and capable of attenuating x-rays without affecting the tactile sensitivity of the hands(12). It is recommended that in the unit evaluated by the present study, the interventional physicians are monitored for their hands, by means of additional dosimeters such as wrist dosimeters, especially during procedures performed through brachial pathway in the continuous fluoroscopy mode.
REFERENCES 1. International Commission on Radiological Protection. Avoidance on radiation injuries from medical interventional procedures. ICRP Publication No. 85. Ann ICRP. 2000;30:7-67. [ ] 2. Padovani R, Rodella CA. Staff dosimetry in interventional cardiology. Radiat Prot Dosimetry. 2001;94:99-103. [ ] 3. Haskal ZJ, Worgul BV. Interventional radiology carries occupational risk for cataracts. RSNA News. 2004;14:5-6. [ ] 4. International Commission on Radiological Protection. Recommendations of the International Commission on Radiological Protection. ICRP Publication No. 60. Oxford: Pergamon Press; 1991. [ ] 5. Brasil. Ministério da Saúde. Diretrizes de proteção radiológica em radiodiagnóstico médico e odontológico. Portaria nº 453. Brasília: Diário Oficial da União nº 100, 1/6/1998. [ ] 6. International Commission on Radiological Protection. Radiological protection and safety in medicine. ICRP Publication No. 73. Ann ICRP. 1996;26:1-47. [ ] 7. Comissão Nacional de Energia Nuclear. Diretrizes básicas de radioproteção. Resolução CNEN nº 27/2004, Norma CNEN-NN-3.01. Rio de Janeiro: CNEN; 2004. [ ] 8. Maurício CLP. Noções de dosimetria termoluminescente: aplicação em dosimetria individual [apostila]. Rio de Janeiro: CNEN; 2001. [ ] 9. Sandborg M, Fransson SG, Pettersson H. Evaluation of patient-absorbed doses during coronary angiography and intervention by femoral and radial artery access. Eur Radiol. 2004;14:653-8. [ ] 10. Tauhata L, Salati I, Di Prinzio R, et al. Fundamentos de radioproteção e dosimetria [apostila]. Rio de Janeiro: CNEN; 2003. [ ] 11. Luz ES, Canevaro LV, Ferreira NMPD, et al. A importância do controle de qualidade em serviços de hemodinâmica e cardiologia intervencionista. Radiol Bras. 2007;40:27-32. [ ] 12. Marx MV, Ellis JH. Radiation protection of the hand in interventional radiology: should it fit like a glove? Radiology. 1996;200:24-5. [ ] Received December 9, 2007. Accepted after revision March 5, 2008. * Study developed at Instituto Nacional de Cardiologia Laranjeiras (INCL), Rio de Janeiro, RJ, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554